Wrist Pathology: Disease and Infection
The hand and wrist may become infected by a variety of causes. Infection frequently follows trauma and can result from bite wounds and other penetrating trauma such as venipuncture and toothpick injuries. Those at risk for hand infection include intravenous drug abusers injecting in the hand with contaminated needles, and diabetics have been shown to have delayed resolution of upper extremity infections. In diabetics, the outcome has been shown to correlate with the depth of infection, as well as the infecting organisms and the underlying renal function. The amputation rate is higher in the presence of a deep infection (fascia, tendon or bone), and if gram negative organisms, anaerobes or multiple microbes are implicated or in the setting of renal failure.
Management of hand infection requires a thorough understanding of the difficulties that result from the virulence of the infecting organisms, the pathways of infection spread and the anatomy of the hand. Direct inoculation of the hand can introduce opportunistic infections, particularly if the hand is exposed to soil or plants. Bite wounds are commonly polymicrobial with mixed aerobic and anaerobic organisms, resulting in severe infection. Other organisms which have been implicated in hand infection include tuberculosis and atypical mycobacteria In fact, the anatomic area most commonly affected by atypical mycobacterium is the region of the hand and wrist. Radiology is essential to delineate the course of infection spread and the anatomy involved, to properly guide medical and surgical management. Superficial infection may be limited to cellulitis; however, the role of imaging is to exclude abscess formation as well as involvement of tendons, deep fascia, bone or joint.
In the hand, tendon sheaths, fascial planes and lymphatics provide a means for infection to spread. Accordingly, digital infection involving the tendon sheath can spread to bones of the affected digit or the wrist. Detection of tendon infection is will guide surgical management . Ultrasound imaging has revealed that tendon enlargement and fluid surrounding the tendon can be identified in suppurative tenosynovitis. Tenosynovitis can be caused by other infectious agents, including tuberculosis and atypical mycobacterium, the latter often the sequela of direct penetrating trauma. MR imaging has demonstrated that mycobacterial tenosynovitis manifests with bursal distention, tendon thickening and rice bodies. These fibrinous soft tissue masses have been identified using MR within the bursa(e) or tendon sheath, and can also be seen in tuberculous infection.
Osteomyelitis may complicate local infection from penetrating wounds or arise from hematogenous dissemination, as occurs with tuberculosis. Tuberculous osteomyelitis can involve the bones of the hand, know has “TB dactyitis”. This usually occurs in children. Radiographic findings include bone destruction, periosteal reaction and later in the course, an expansile lytic lesion referred to as “spina ventosa”. Tuberculous and other fungal osteomyelitis typically crosses the physis, as opposed to pyogenic infections which do not. Accordingly, identification of infection crossing the physis should raise concern for these organisms.
Septic arthritis is uncommon in the hand. However, early diagnosis is imperative. This usually arises secondary to bite wounds or other penetrating trauma.
 |  |  |  |
 |  |  |  |
 |  |  |  |
 |  | ||
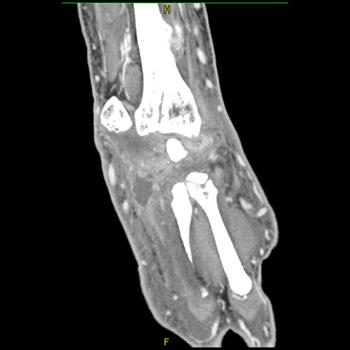
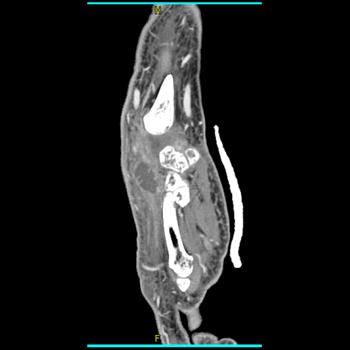
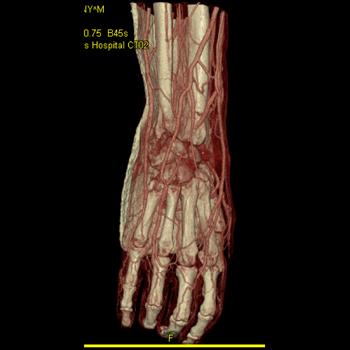
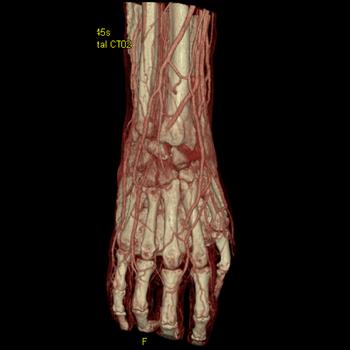
Clinical History: CT Findings: Diagnosis: Wrist abscess Outcome: Comments: | |||