Wrist Pathology: Scaphoid Fractures
Of the carpal bones, the scaphoid is the most common to fracture, accounting for 60-70% of carpal bone fractures. It is the second most common site of fracture in the wrist. The most frequent type of fracture is through the waist, comprising 66-70%. The proximal pole is the second most common location, involved in 20% of scaphoid fractures. Other sites of fracture include the distal body, tuberosity and distal articular region. The prognosis is impacted by the location, with distal fractures having a better outcome. Proximal pole fractures are associated with delayed union and nonunion.
The early detection of scaphoid fractures is essential, but can be challenging. The positive predictive value of physical examination findings has been reported to range from13-69%. In the setting of high clinical suspicion, the negative predictive value of a radiograph is 50-87%. Delayed detection is one of the factors contributing to nonunion and can wrist dysfunction. The literature describes a false negative rate of up to 44% for detecting scaphoid fractures on conventional radiographs. CT, MR and ultrasound have each been advocated to detect clinically suspected fractures not evident on conventional radiographs. Recently, MR has been shown to be sensitive, specific and accurate and cost effective as a screening tool in cases with a high suspicion but negative radiograph.
Prior to MDCT, direct acquisition of data along coronal or sagittal-oblique planes were advised to best evaluate the scaphoid for fracture. The sagittal oblique acquisition was recommended using a wrist holder and with the wrist pronated. Because the majority of waist fractures run parallel to the axial axis or mid-oblique, coronal or sagittal-oblique scans will acquire data perpendicular to the fracture line. Following treatment, a 40 degree angled coronal CT has been advocated to improve the quality of the dataset in patients with plaster and fiberglass casts. Because MDCT datasets are isotropic, an axial acquisition will result in a dataset which can be evaluated in coronal and sagittal orientations with no loss of resolution. An important topic for future investigation is whether axial MDCT with .5 mm collimation can overcome the limitations of spiral CT which warranted the alternative planes of acquisition and wrist positioning.
Indications for CT include high clinical suspicion with a negative radiograph, equivocal radiograph findings, comprehensive evaluation for angulation and displacement in the setting of a fracture, follow up assessment for healing and union, as well as post-operative imaging. The conventional radiograph can not always provide a complete evaluation due to obscuration of the scaphoid by the other carpal bones. Furthermore, if the radiograph demonstrates excessive dorsal tilt of the lunate, CT is required to exclude displacement of a scaphoid waist fracture. Dorsal tilt can be secondary to scaphoid waist fracture displacement as well as intercarpal ligament injury. Furthermore, the presence of dorsal tilt of the lunate has been shown to correlate with malunion and nonunion in 83% of cases. An additional radiographic finding which would prompt further evaluation with CT is the presence of scaphoid lucencies. In a small percentage of scaphoid fractures (.3%), lucencies within the scaphoid bone were detected with no fracture line apparent on the radiograph. On CT, a fracture line was evident. These pseudocysts are hypothesized to arise secondary to ischemia, and indicate nonunion of scaphoid microfractures.
Determination of whether a scaphoid fracture is stable or unstable is important parameter well suited by the high resolution of MDCT. The reported incidence of instability is 30-40%. By definition, instability is present if stress radiographs demonstrate interfragmentary movement or if the fracture is displaced more than 1 mm. Determination of such a small degree of displacement is facilitated by CT datasets with .5 mm collimation.
A number of complications have been described following fracture of the scaphoid bone. These include delayed union, nonunion, malunion (dorsal humpback), AVN, carpal instability, osteoarthritis, carpal tunnel syndrome and sympathetic dystrophy.
Malunion can manifest as a “dorsal humpback deformity”. This finding is not always apparent on conventional radiographs due to obscuration by overlying bones. Owing to palmar angulation of the distal fracture fragment, the dorsal surface of the bone develops a bony prominence. Complications of this deformity include radiocarpal osteoarthritis and functional impairment.
Avascular necrosis of the proximal fragment is a well known sequela which is a factor contributing the incidence of nonunion. The incidence is 10-15% for all scaphoid fractures and 30% after waist fractures. This unfortunate complication results from the fact that the majority of the blood supply to the scaphoid enters through the distal portion of the bone. The most common type of fracture, a transverse or oblique waist fracture, can disrupt the blood supply to the proximal fragment. Prior to MR, the determination of the vascularity of the proximal fragment was attempted with conventional radiographs, bone scintigraphy and CT. Nuclear medicine has been shown to have a low specificity and is limited by poor resolution. A study comparing MR to surgery demonstrated 66% sensitivity, 88% specificity and 83% accuracy using gadolinium enhanced MR to determine the vascularity of the proximal pole in cases of nonunion.
On radiographs and CT, AVN is indicated by increased density of the bone A study by Downing compared conventional radiographs 8 weeks following the fracture and high resolution helical CT at 12 weeks. Correlation was made with bone enhancement at gadolinium enhanced MR and rate of union at follow up. The results showed non significant association between “definitely increased density” on radiographs and diminished blood flow at MR. Radiographs are limited in specificity, as increased density can result from proximal pole rotation and new bone deposition. A correlation was found between “definitely increased density” at CT and decreased gadolinium enhancement. However, neither CT nor radiograph findings suggesting AVN were associated with the rate of fracture nonunion.
Nonunion has been reported in 5% of treated scaphoid fractures and in 33-55% of unstable fractures. Determination of whether a scaphoid fracture has united is better served by CT than radiographs. CT is more sensitive for detecting bone bridging and for identifying focal regions of nonunion within proliferative bone. Nonunited scaphoid fractures have been classified by the type of displacement (volar vs. dorsal), which has been shown to correlate with the fracture location (proximal vs. distal to the dorsal apex of the ridge of the scaphoid). Volar displacement is present when the distal fragment overlaps the proximal fragment volarly, and dorsal displacement when the overlap occurs dorsally. CT with 3D reconstructions was performed on nonunited scaphoid fractures and the fracture location was shown to correlate with the type of displacement. Distal fractures were associated with volar type nonunion, and this type of nonunion had a 100% incidence of DISI. Dorsal type nonunions were associated with proximal fractures, and only 30% developed DISI. In addition, the 3D renderings were used for proximity mapping of the distances between the bones. The results showed a change in the radiocarpal contact areas in association with dorsal type displacement.
Treatment of nonunion requires internal fixation with a bone graft. Following surgery, a number of parameters have been identified which may predict a poor outcome. These include the size of the proximal fragment, the presence of proximal AVN, the degree of fracture displacement and the mechanism by which the bone is grafted. Nonunion leads to radioscaphoid and wrist arthritis. The duration of the nonunion, the degree of fracture displacement and the presence of carpal instability (defined as more than 10 degrees of lunate dorsiflexion) all impact the development of arthritis following a scaphoid fracture. Accordingly, attention should be paid to identification and reporting of these associated findings when performing CT.
 | 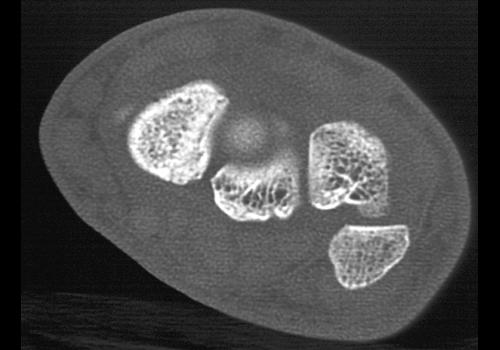 |  |  |
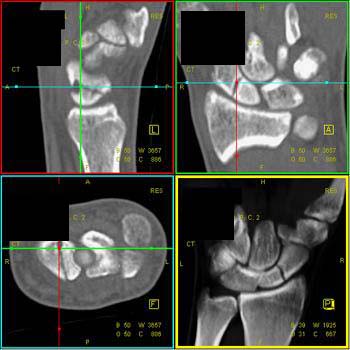
Clinical History: 21 year old man who fell on his right outstretched hand one year prior.He complains of pain with activity at his right dorsal wrist. CT Findings: The study demonstrates non-union. Diagnosis: Scaphoid fracture. Outcome: The patient was placed in cast and treated conservatively. Comments: Initial considerations was that of avascular necrosis but none was subsequently proven. | |||
 |  |  |  |
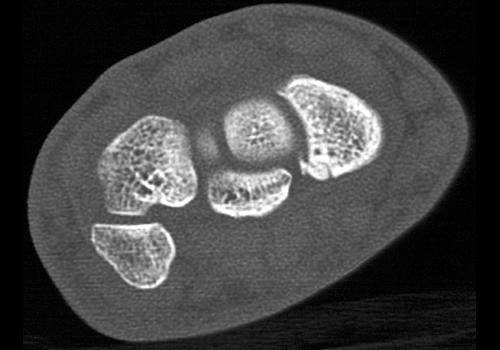
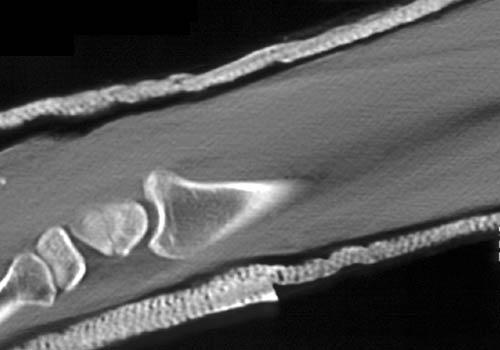
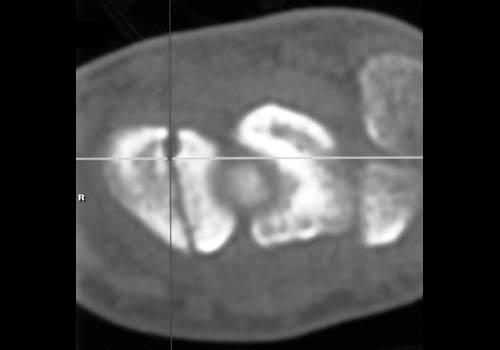
Clinical History: The patient had recent trauma with persistent pain over the wrist. CT Findings: A subtle scaphoid fracture is seen representing a small chip fracture. Diagnosis: Scaphoid fracture. Outcome: Comments: Best defined on 0.5 mm high resolution scans using a bone algorithm. | |||
 |  |  |  |
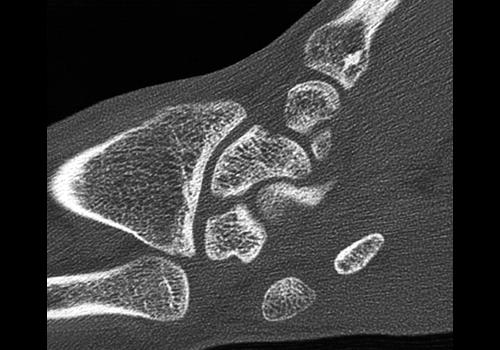
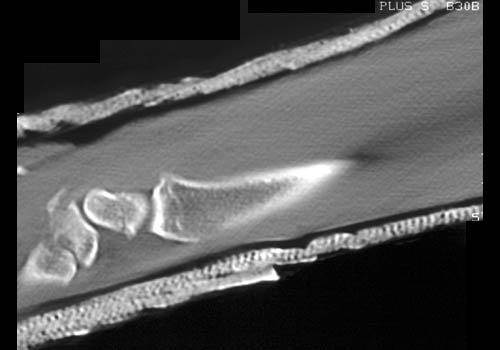
Clinical History: CT Findings: Transverse fracture of the mid scaphoid, with persistant separation of fracture fragments. Diagnosis: Non-union of the scaphoid. Outcome: Comments: Proximal fragment is at risk for avascular necrosis due to interruption of blood supply. | |||
 |  | ||
Clinical History: CT Findings: Diagnosis: Repair of scaphoid fracture. Outcome: Comments: | |||
 |  |  |  |
Clinical History: CT Findings: Comminuted fracture involving the distal radius, extending into the articular surface with the carpal bones. The proximal and distal fracture fragments are impacted. Diagnosis: Fracture of the scaphoid. Outcome: Comments: | |||
 |  |  | |
Clinical History: 38 year old male. CT Findings: Transverse left scaphoid fracture. Diagnosis: Scaphoid fracture. Outcome: Comments: | |||
 |  |  |  |
 |  |  | |
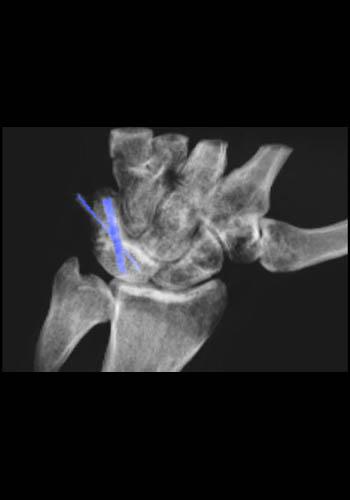
Clinical History: 22 year old male with history of scaphoid fracture. CT was obtained to evaluate healing. CT Findings: Volume rendered 3D CT image of the wrist shows a non-displaced fracture of the body of the scaphoid. There is no evidence of healing at this time. Diagnosis: Scaphoid fracture. Outcome: Comments: | |||