Wrist Anatomy Quiz
1. Which of the following is true with respect to multiplanar imaging of the wrist?


B. the best orientation for imaging the scaphoid is axial
C. the hook of the hamate is best evaluated in the axial plane
D. all of the above
E. A and C
Correct! Incorrect. The correct answer is E.
2. Why is CT imaging essential in determining the outcome of a distal radius fracture?
B. CT has been shown to be superior for measuring the articular gapping, with substantially larger measurements compared to radiographs
C. The presence of articular incongruities measuring more than 1-2 mm after closed reduction is felt by many to be an indication for surgical reduction to prevent disabling osteoarthritis and maintain wrist function
D. All of the above
Correct! Incorrect. The correct answer is D.
3. Which of the following is false with respect to ulnar styloid fractures:

B. they are associated with injuries of the TFCC and ligamentous injuries
C. they are of no value in predicting the development of DRUJ instability
D. all of the above
E. A and C
Correct! Incorrect. The correct answer is E.
4. Complications of distal radius fractures include

B. nerve compression and pain syndromes
C. infection, including osteomyelitis
D. osteoarthritis of the wrist
E. all of the above
Correct! Incorrect. The correct answer is E.
5. Regarding the detection of scaphoid fractures:
B. In the setting of high clinical suspicion, the negative predictive value of a radiograph is 50-87%
C. The literature describes a false negative rate of up to 44% for detecting scaphoid fractures on conventional radiographs
D. CT, MR and ultrasound have each been advocated to detect clinically suspected fractures not evident on conventional radiographs
E. All of the above.
Correct! Incorrect. The correct answer is E.
6. Which of the following is true with respect to AVN of the scaphoid:

B. AVN results from the fact that the majority of the blood supply to the scaphoid enters through the distal portion of the bone, and the most common type of fracture, a transverse or oblique waist fracture, can disrupt the blood supply to the proximal fragment
C. Research has demonstrated that increased bone density of the proximal fragment on radiographs does not correlate well with diminished vascularity at gadolinium enhanced MRI
D. A correlation has been shown between "definitely increased density" at CT and decreased gadolinium enhancement on MRI
E. All of the above
Correct! Incorrect. The correct answer is E.
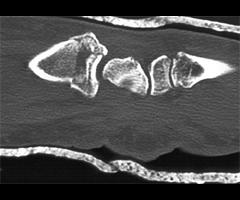
7. Which of the following is true with respect to the imaging findings on this CT of the scaphoid?

B. The findings definitively reflect fracture through a congenital scaphoid cyst
C. The lucency could represent ischemia
D. If such a lucency is seen on a radiograph without a fracture, it should be interpreted as a congenital cyst with no further imaging
E. A and C
Correct! Incorrect. The correct answer is E.
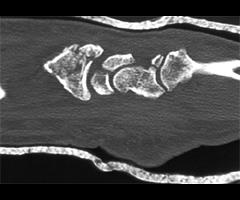
8. Which of the following is true with respect to malunion of this type of fracture?

B. may be radiographically apparent, but has no impact on the patient's outcome
C. should be suspected if a dorsal bony prominence in seen on CT
D. is usually apparent on conventional radiographs
E. All of the above
Correct! Incorrect. The correct answer is C.
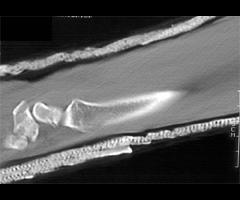
9. Which of the following is true with respect to the fracture depicted in this image?:
B. this type of injury is usually due to direct trauma by swinging the handle of a baseball bat, golf club or tennis racquet
C. traditional radiographic views of the wrist are usually insufficient to identify this fracture
D. diagnosis is important because the ulnar nerve travels near the hook, and neurologic damage can result from the motion of an ununited fracture
E. All of the above
Correct! Incorrect. The correct answer is E.
10. Which of the following is true with respect to the category of pathology demonstrated by these 2 cases?
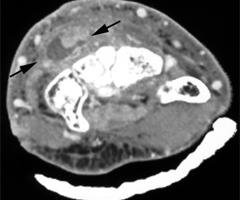

B. Diabetics have been shown to have delayed resolution
C. Rice bodies can be seen in tendinous involvement by mycobacteria
D. Imaging is essential to define the extent and the involved anatomy
E. All of the above
Correct! Incorrect. The correct answer is E.