Wrist Pathology: Distal Radial Fractures
The distal radius is most commonly fractured in older women, particularly those with osteoporosis. The younger patient may sustain a distal radius fracture in the setting of severe trauma. In many cases, these fractures are readily apparent on conventional radiographs. However, subtle fracture may not be evident, and CT should be considered to detect these in patients with a high clinical suspicion and a negative radiograph. CT provides a comprehensive evaluation of distal radius fractures and has been shown to impact treatment plans for intra-articular radial fractures.
Goldfarb's article entitled “CT of the wrist: What the clinician wants to know” provides an outstanding overview of how radiologists should approach wrist fractures. He provides a thorough summary of the classification systems for distal radius fractures. Most importantly, he clearly elucidates the specific findings which must be detailed in the evaluation of distal radius fractures. The following features should be described: the type of fracture (transverse, oblique, depressed), angulation, displacement, presence of comminution, intraarticular extension (radiocarpal or distal radio-ulnar joint, evidence of ligamentous injury and the presence and location of an unlar styloid fracture.
Intra-articular extension is reported to occur in 50-81% of distal radius fractures. If identified, a detailed description of the location and appearance must be provided. The radiocarpal articulation (at the scaphoid and lunate fossa), the radioulnar articulation (at the sigmoid notch) or the ulnar styloid may be involved. Careful inspection must be made to detect any step-off in the articular region of the radiocarpal joint or gaps, because these have prognostic value for the development of radiocarpal osteoarthritis. The presence of articular incongruities measuring more than 1-2 mm after closed reduction is felt by many to be an indication for surgical reduction to prevent disabling osteoarthritis an d maintain wrist function. CT has been shown to be superior for measuring the articular gapping, with substantially larger measurements compared to radiographs. Furthermore, radiographs underestimate the degree of comminution and DRUJ involvement. With respect to articular step-offs, one study by Katz showed no significant difference between CT and radiographs for quantification; however, Pruitt demonstrated that determination of t he extent of articular surface depression was better with CT.
An ulnar styloid fracture is present in 51-65% of distal radius fractures. Fractures of ulnar styloid are important to identify and localize because of the associated ligamentous injuries. The triangular fibrocartilage complex (TFCC) attaches to the ulnar styloid, and the dorsal and volar radioulnar ligaments attach to the base. The fracture size and the degree of displacement both correlate with the development of DRUJ instability. In ones series, all distal radius fractures which developed DRUJ dysfunction had a concomitant ulnar styloid fracture. Fractures of the base had the highest incidence of DRUJ instability.
A long list of potential complications have been reported following a distal radius fracture. In addition to delayed union, malunion and nonunion, patients may suffer from loss of motion, nerve compression and pain syndromes like RSD. Complications can arise relating to indwelling hardware, including infection. Additional complications include carpal instability, osteomyelitis, tendon inflammation, dysfunction or rupture, ligament damage, contractures, arthritis, and DRUJ dysfunction. Knowledge of these should guide the evaluation of post operative films in patients with distal radius fractures.
Extraarticular malunion of distal radius fractures manifests by number of factors, which can be identified with CT and should be assessed by the radiologist both pre and post reduction. These findings may dictate the need for surgical reduction if they are present following closed reduction. Radial shortening results in DRUJ osteoarthritis and DRUJ dysfunction. As little as 2.5 mm will increase the ulnar load, and 6 mm results in clinical symptoms. A decrease in radial inclination (more than 5 degree loss) contributes to DRUJ dysfunction. A change in the volar tilt is an additional parameter. A loss of volar tilt of more than 10 degrees is felt to be an indication for reduction. This angulation also increases ulnar load and impacts DRUJ mechanics.
For intraarticular malunion, the most significant factor is articular incongruity. Gap displacement or the presence of step-off displacement contribute to the development of osteoarthritis. Following closed reduction, if displacements of more than 1-2 mm are identified, surgery is commonly performed. Because helical CT has been shown to be superior to radiographs for quantitization of these gaps, narrow collimation MDCT should provide even more accurate measurements such small regions of diastasis, regardless of the fracture orientation.
 |  |  | 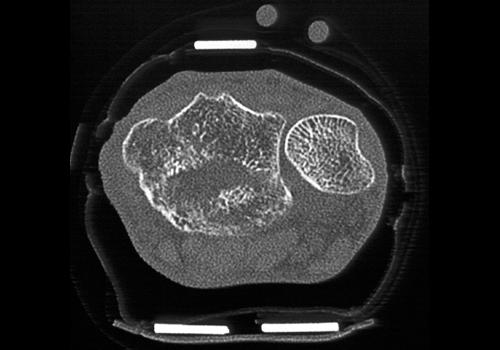 |
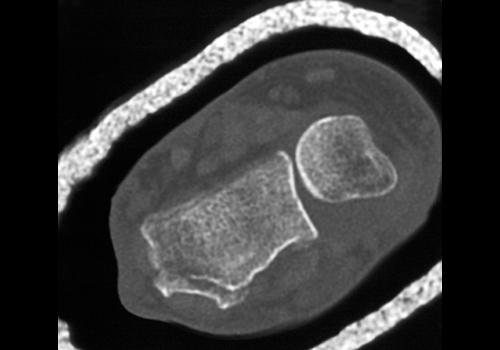
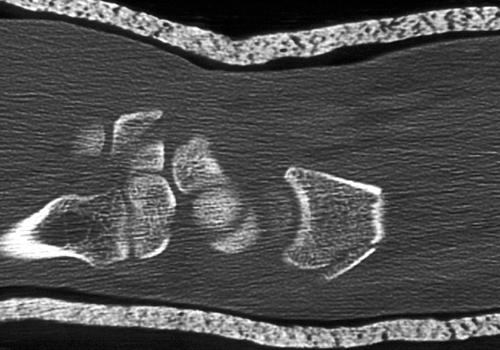
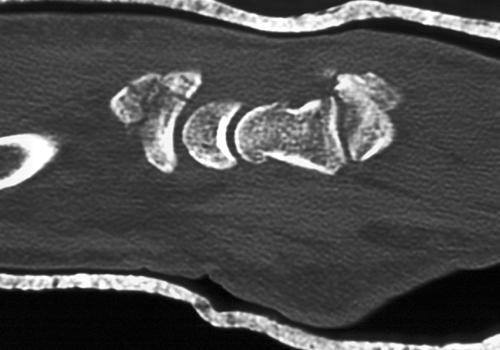
Clinical History: The patient fell off his bike and obtained a distal radius fracture of the Smith type. CT Findings: distal radius fracture of the Smith type. Diagnosis: Distal radius fracture of the Smith type. Outcome: Due to the extent of the fracture the patient underwent open reduction with internal fixation. The patient recovered satisfactorily. Comments: | |||
 |  |  |  |
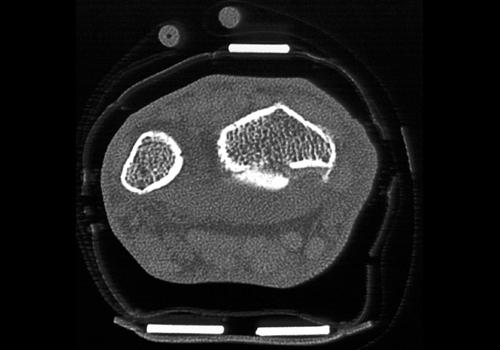
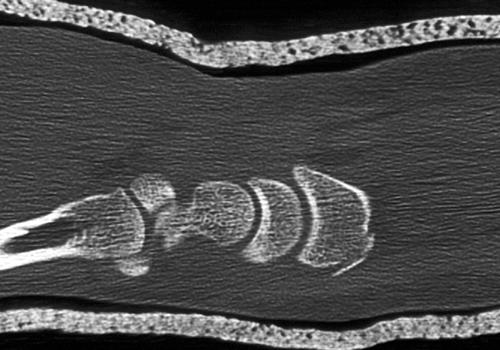
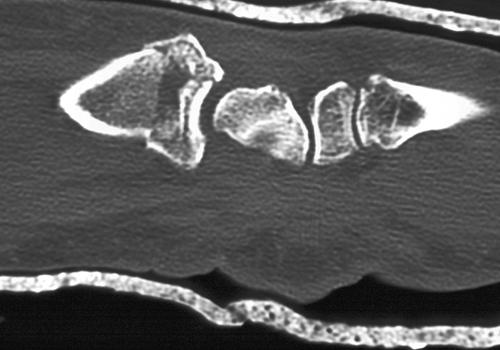
Clinical History: Patient presents with pain after fall.. CT Findings: Scans demonstrate degenerative osteoarthritis in this 73-year-old female. The study also demonstrates a distal radial fracture due to a recent fall. Diagnosis: Degenerative osteoarthritis and distal radial fracture. Outcome: The patient was treated with splint immobilization. Comments: | |||
 |  | 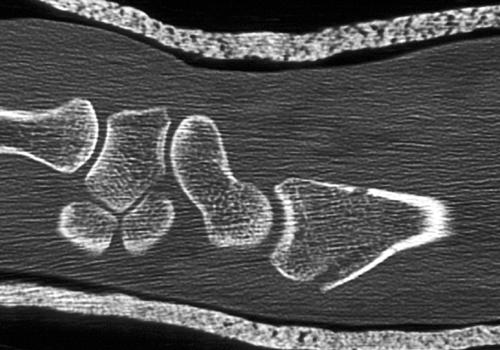 |  |
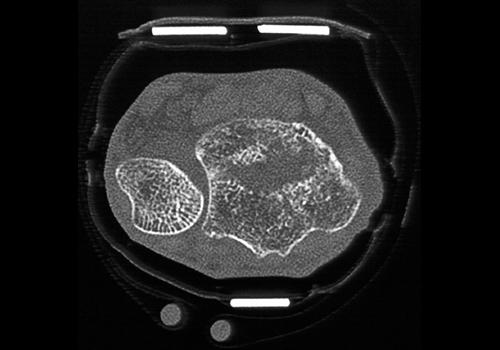
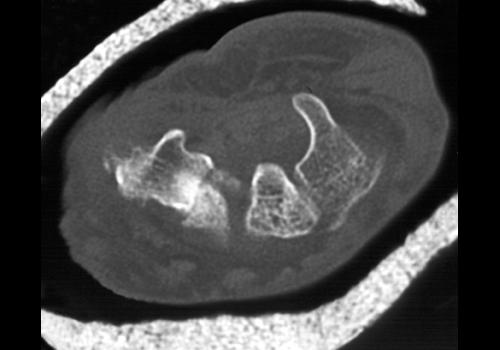
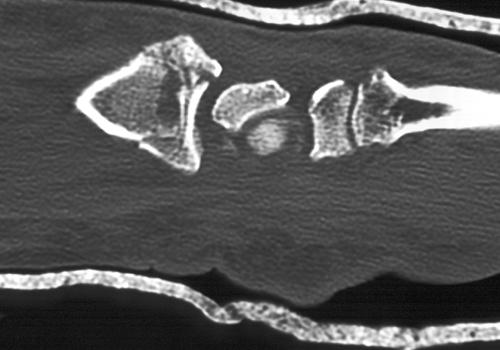
Clinical History: The patient was in a motor vehicle accident as a pedestrian and had a comminuted fracture of the distal radius. CT Findings: Comminuted fracture of the distal radius. Diagnosis: Fracture of the distal radius. Outcome: The patient was treated conservatively. Comments: The carpal bones were intact. | |||
 |  |  | 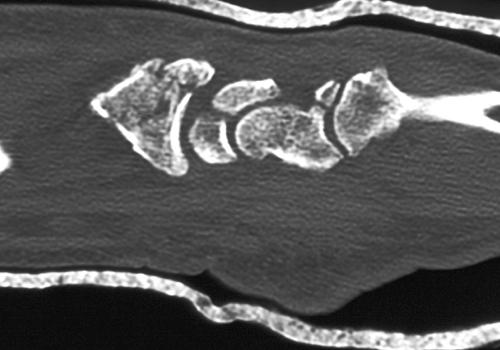 |
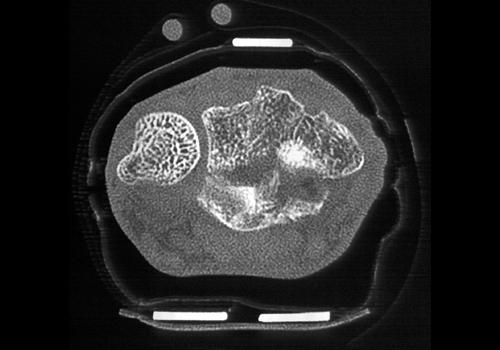
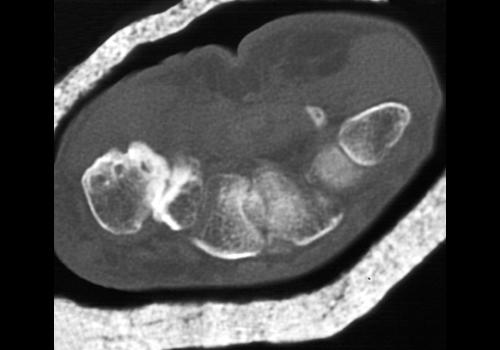
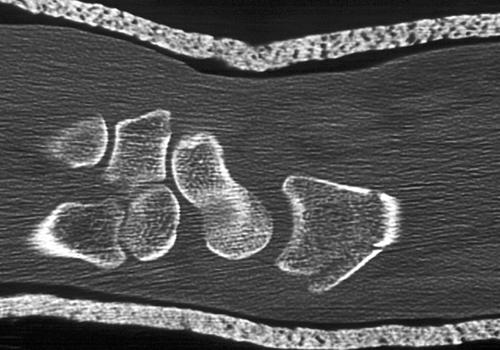
Clinical History: The patient fell on his wrist and has evidence of an impacted distal radial fracture. CT Findings: The relationship to the carpal bones appears to be intact despite the comminuted nature of the fracture and the fracture’s interarticular extension. Diagnosis: Distal radial fracture. Outcome: Post reduction was performed because of the extent of injury with percutaneous pinning with iliac crest bone graft. The patient recovered without complication. Comments: | |||
 |  |  |  |
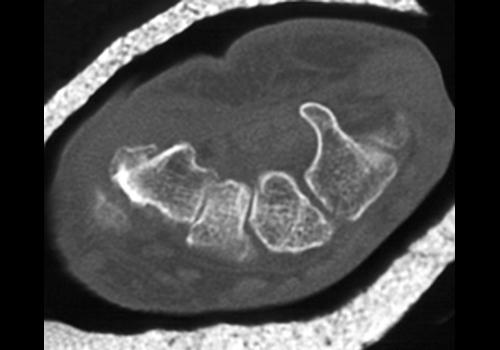
Clinical History: CT Findings: Severely comminuted fracture of the distal radius. Mild displacement and angulation of fracture fragements noted. Diagnosis: Fracture of the radius. Outcome: Comments: The 4th image is a volume rendered 3D reconstruction. | |||
 |  | ||
Clinical History: CT Findings: Comminuted fracture of the distal radius, involving the articular surface with the carpal bones. Mild periosteal reaction medially. The ulnar styloid is avulsed. Diagnosis: Fracture of the radius. Outcome: Comments: | |||
 |  |  |  |
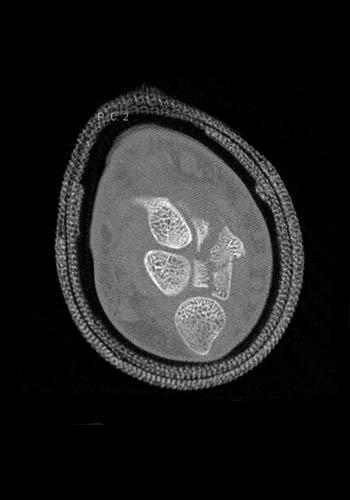
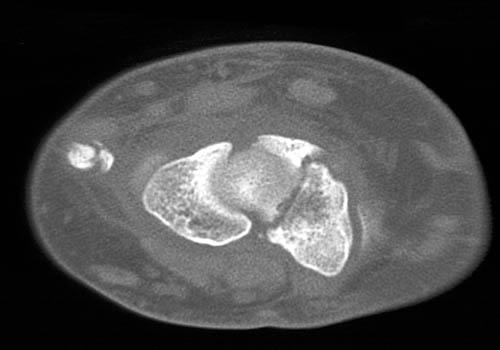
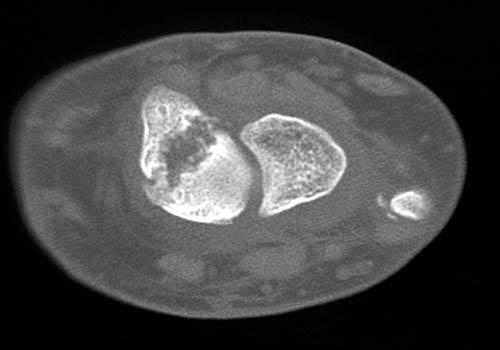
Clinical History: CT Findings: Comminuted fracture involving the distal radius, extending into the articular surface with the carpal bones. The proximal and distal fracture fragments are impacted. Diagnosis: Fracture of the radius. Outcome: Comments: | |||
 |  |  |  |
 | |||
Clinical History: 15 year old boy who fell on wrist playing football. CT Findings: Salter Harris II fracture of the right distal radius with large dorsal Thurston-Holland fragment. Diagnosis: Salter Harris II fracture right distal radius. Outcome: Open reduction and internal fixation right distal radius. Comments: | |||