|
-- OR -- |
|
- “The kidney is the most common solid organ transplant globally and rates continue to climb, driven by the increasing prevalence of end stage renal disease (ESRD). Compounded by advancements in surgical techniques and immunosuppression leading to longer graft survival, radiologists evermore commonly evaluate kidney transplant patients and candidates, underscoring their role along the transplant process. Multiphase computed tomography (CT) with multiplanar and 3D reformatting is the primary method for evaluating renal donor candidates, detailing renal size, vascular/collecting system anatomy, and identifying significant pathologies such as renal vascular diseases and nephrolithiasis.”
Radiologic evaluation of the kidney transplant donor and recipient.
Goiffon RJ, Depetris J, Dageforde LA, Kambadakone A.
Abdom Radiol (NY). 2024 Jul 10. doi: 10.1007/s00261-024-04477-4. Epub ahead of print. PMID: 38985292. 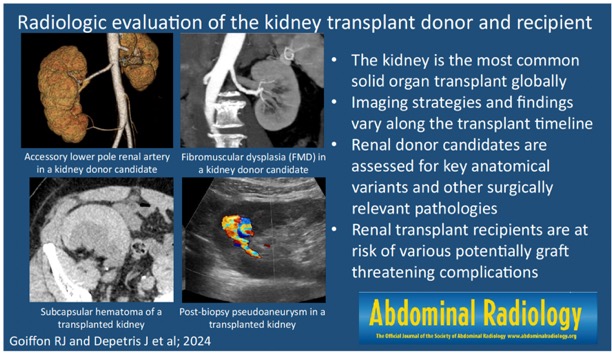
Radiologic evaluation of the kidney transplant donor and recipient.
Goiffon RJ, Depetris J, Dageforde LA, Kambadakone A.
Abdom Radiol (NY). 2024 Jul 10. doi: 10.1007/s00261-024-04477-4. Epub ahead of print. PMID: 38985292.- 3D images created by a technologist are useful to referring clinicians without PACS access to help conceptualize the spatial relationships between the anatomic structures. These can include curvilinear planes following key vessels, maximum intensity projections (MIPs) showing singleimage vascular relationships, and 3D rendered rotating anatomic models. The choice of images sent to the EMR must be made in context of referring transplant team’s expectations as well as 3D technologist availability or, without this resource, the time and technology constraints of the radiologist.
Radiologic evaluation of the kidney transplant donor and recipient.
Goiffon RJ, Depetris J, Dageforde LA, Kambadakone A.
Abdom Radiol (NY). 2024 Jul 10. doi: 10.1007/s00261-024-04477-4. Epub ahead of print. PMID: 38985292. - “Modern helical, multidetector CT data can create volumetric, thin-slice images to allow for multiplanar reconstruction (MPR) by the interpreting radiologist on the picture archive and storage (PACS) system. While this obviates the need for separate coronal and sagittal images for the radiologist, 3 mm thick coronal and sagittal images are still usually sent to PACS for viewing in the electronic medical record (EMR) by the transplant team. These thicker coronal and sagittal images are not adequate to detect subtle but important findings such as vasculopathies, ostial calcifications, and small renal stones due to the Nyquist sampling theorem.”
Radiologic evaluation of the kidney transplant donor and recipient.
Goiffon RJ, Depetris J, Dageforde LA, Kambadakone A.
Abdom Radiol (NY). 2024 Jul 10. doi: 10.1007/s00261-024-04477-4. Epub ahead of print. PMID: 38985292. - “Renal length should be measured using MPR images aligned to the principal and secondary orthogonal long axes, given that kidneys often lie obliquely, making coronal measurements unreliable. Kidney length is a poor predictor of renal function so parenchymal or cortical volumes should also be reported—both are valid as proxies for renal function —as assessed by the radiologist, a 3D technologist, or automated segmentation software. These volumes are used to estimate split function for triaging which kidney to donate, as current published data are too preliminary to support an absolute renal volume cutoff for transplantation.”
Radiologic evaluation of the kidney transplant donor and recipient.
Goiffon RJ, Depetris J, Dageforde LA, Kambadakone A.
Abdom Radiol (NY). 2024 Jul 10. doi: 10.1007/s00261-024-04477-4. Epub ahead of print. PMID: 38985292. - “Fibromuscular dysplasia (FMD) is a non-inflammatory vasculopathy affecting medium to large vessels, predominantly diagnosed in middle-aged females, and most commonly involving the renal arteries. This condition can lead to dissections, aneurysms, and stenosis and is likely underdiagnosed due to its imaging similarities with atherosclerosis and its tendency to be asymptomatic . On CT, FMD can present as beading from alternating strictures and aneurysms, long smooth stenoses from thrombosed dissections, or fenestrated dissection flaps .Mild FMD may be challenging to detect on CT and can progress post-transplant to disease threatening renal function, making it a conundrum when approving renal donors.”
Radiologic evaluation of the kidney transplant donor and recipient.
Goiffon RJ, Depetris J, Dageforde LA, Kambadakone A.
Abdom Radiol (NY). 2024 Jul 10. doi: 10.1007/s00261-024-04477-4. Epub ahead of print. PMID: 38985292. - “Kidney transplantation is increasing in the United States and abroad, emphasizing the need for radiologists to know best practices of donor and post-transplant recipient evaluation. Transplant patient assessment is multidisciplinary; radiologists gain from knowing the surgical approach of donor nephrectomy and implications of post-operative complications to better communicate with referring transplant surgeons. Knowledge of the clinical manifestations of imaging findings aids radiologists in adjusting pre-test probabilities and prompting additional imaging if initial studies are inadequate. With the recent introduction of genetically modified renal xenografts as a promising solution to the organ shortage, familiarity with transplant imaging may become further vital to the radiologist.”
Radiologic evaluation of the kidney transplant donor and recipient.
Goiffon RJ, Depetris J, Dageforde LA, Kambadakone A.
Abdom Radiol (NY). 2024 Jul 10. doi: 10.1007/s00261-024-04477-4. Epub ahead of print. PMID: 38985292.

- “Despite the theoretical risk from ionizing radiation, CT is preferred over MR because of its higher spatial resolution and speed, and because it is less prone to artifacts. Compared to CT, MR angiography is much more prone to motion-related artifacts. Vascular calcification and urolithiasis are better depicted by CT than MR.”
CT evaluation of the renal donor and recipient Vernuccio F et al. Abdom Radiol (2018) (in press) - “Common reasons for potentially excluding a donor based on CT findings include renal anatomic variability (i.e., unilateral renal agenesis, renal ectopia, horseshoe kidney), complex vascular anatomy, urolithiasis, and malignancy. The presence of multiple renal arteries is considered a relative contraindication owing to longer operative times and higher risk of arterial thrombosis. Abnormalities of the collecting sys- tem might contraindicate transplant, including severe hydronephrosis, papillary necrosis, transitional cell carcinoma, or important anatomical variants such as ureteric duplication or ureteropelvic junction obstruction.”
CT evaluation of the renal donor and recipient Vernuccio F et al. Abdom Radiol (2018) (in press) - “All measurements should be performed in the corti- comedullary phase. Kidney volume can be calculated by manually tracing the renal cortex on each image showing renal parenchyma and excluding the renal pelvis or it can be automatically estimated from bidimensional kidney measurements on axial images using predefined formulas. More recently, kidney volume can be measured with semiautomated or automated segmentation techniques that do not require manual tracing of the edges of the kidneys.”
CT evaluation of the renal donor and recipient Vernuccio F et al. Abdom Radiol (2018) (in press) - “The vascular renal assessment is mandatory consid- ering that certain vascular anomalies may disqualify a potential donor. Arterial assessment is performed in the arterial phase and includes anatomic information with standardized measurements, delineation of vascular variants , and assessment for vascular diseases. In most individuals, the main renal artery originates between the upper margin of the L1 and the lower margin of the L2 vertebrae, with the right renal artery usually originating above the left renal artery with respect to the vertebral column.”
CT evaluation of the renal donor and recipient Vernuccio F et al. Abdom Radiol (2018) (in press)
- “Excellent interobserver agreement was noted for each calcification score category. The common iliac arteries showed significantly higher average calcification scores than the external iliac arteries for all categories. Advanced age and diabetes mellitus were independently predictive of higher scores in each category, whereas hypertension, cigarette smoking, hyperlipidemia, and sex were not. Based on multivariate analysis, only the calcification morphology score of the arterial segment used for anastomosis was independently predictive of a higher rate of surgical complexity and of DGF. None of the scores was predictive of graft or patient survival. However, patients with CT evidence of iliac arterial calcification had a lower 1-year survival after transplant than those who did not (92% vs 98%, respectively; p = 0.05).”
Application of a Novel CT-Based Iliac Artery Calcification Scoring System for Predicting Renal Transplant Outcomes Davis B et al. AJR 2016; 206:436–441 - “Excellent interobserver agreement was noted for each calcification score category. The common iliac arteries showed significantly higher average calcification scores than the external iliac arteries for all categories. Advanced age and diabetes mellitus were independently predictive of higher scores in each category, whereas hypertension, cigarette smoking, hyperlipidemia, and sex were not. Based on multivariate analysis, only the calcification morphology score of the arterial segment used for anastomosis was independently predictive of a higher rate of surgical complexity and of DGF. None of the scores was predictive of graft or patient survival. However, patients with CT evidence of iliac arterial calcification had a lower 1-year survival after transplant than those who did not (92% vs 98%, respectively; p = 0.05).”
Application of a Novel CT-Based Iliac Artery Calcification Scoring System for Predicting Renal Transplant Outcomes Davis B et al. AJR 2016; 206:436–441 - “Excellent interobserver agreement was noted for each calcification score category. The common iliac arteries showed significantly higher average calcification scores than the external iliac arteries for all categories. Advanced age and diabetes mellitus were independently predictive of higher scores in each category, whereas hypertension, cigarette smoking, hyperlipidemia, and sex were not. Based on multivariate analysis, only the calcification morphology score of the arterial segment used for anastomosis was independently predictive of a higher rate of surgical complexity and of DGF. None of the scores was predictive of graft or patient survival.”
Application of a Novel CT-Based Iliac Artery Calcification Scoring System for Predicting Renal Transplant Outcomes Davis B et al. AJR 2016; 206:436–441
- “ Renal parenchymal and vascular abnormalities are common in asymptomatic potential renal donors. Although most of these represent incidental CT findings, abnormalities can exclude potential renal donors and alter the surgical approach in a small minority of cases.”
Role of MDCT Angiography in Selection and Presurgical Planning of Potential Renal Donors
Chu LC, Sheth S, Segev DL, Montgomery RA, Fishman EK
AJR 2012; 199:1035-1041 - “ Although renal and extrarenal abnormalities were present in 41% of potential renal donors abnormalities seen on CT only contributed to exclusion of 27 potential donors (4.1%). The most common reason for exclusion was the presence of renal masses or scarring (1.8%).”
Role of MDCT Angiography in Selection and Presurgical Planning of Potential Renal Donors
Chu LC, Sheth S, Segev DL, Montgomery RA, Fishman EK
AJR 2012; 199:1035-1041 - “ The most common renal abnormalities were cysts (34%) and renal stones (4.4%). Renal artery disease was identified in 3.4% of potential donors, including renal artery stenosis, possible fibromuscular dysplasia, and renal artery aneurysm. Suspicious renal masses was incidentally found in 0.5% of potential donors.”
Role of MDCT Angiography in Selection and Presurgical Planning of Potential Renal Donors
Chu LC, Sheth S, Segev DL, Montgomery RA, Fishman EK
AJR 2012; 199:1035-1041
- “ Studies using angiography have revealed that 3.8%-6.6% of potential renal donors have fibromuscular dysplasia (FMD), which was bilateral in 43% to 71%. Atherosclerotic lesions were much less common, identified in 2%.”
Computed Tomography Angiography of the Renal and Mesenteric Vasculature: Concepts and Applications
Johnson PT, Fishman EK
Seminars in Roentgenology
2011: 115-124
- CT Angiography of the Renal Arteries: Renal Donor Evaluation
-Number and location of the renal arteries including presence of prehilar branching
-Detection of renal artery stenosis and fibromuscular dysplasia (FMD)
-Presence of renal mass or other important renal findings (horseshoe kidney, scarring of the kidney)
-Renal vein and collecting system also evaluated on venous and delayed topogram "Of these, 94 (0f 199) were rejected for donation, with 15 rejected on the basis of multidetector CT findings (bilateral renal atheromatosis or fibromuscular dysplasia in six cases, unsuspected abdominal tumors in four cases, and multiple renal artery or vein pedicles in five cases)."
Multidetector CT of Living Renal Donors: Lessons Learned From Surgeons
Sebastia C et al
RadioGraphics 2010; 30;1875-1890"Knowledge of the surgical technique used and the difficulties that surgeons may face during laparoscopic nephrectomy and subsequent renal transplantation is essential to compile accurate radiologic reports."
Multidetector CT of Living Renal Donors: Lessons Learned From Surgeons
Sebastia C et al
RadioGraphics 2010; 30;1875-1890"Some limitations to our study must be acknowledged. Renal neoplasms may not be evident in the early corticomedullary phase."
Combined Vascular-Excretory Phase MDCT Angiography in the Preoperative Evaluation of Renal Donors
Zamboni GA et al.
AJR 2010; 194:145-150"Furthermore,only vascular abnormalities were detected in our patients, and no renal parenchyma abnormalities were observed."
Combined Vascular-Excretory Phase MDCT Angiography in the Preoperative Evaluation of Renal Donors
Zamboni GA et al.
AJR 2010; 194:145-150"Using a split-bolus injection of contrast medium and an arterial phase acquisition, we can produce CTA images that provide information from the arterial, venous, parenchymal, and excretory phases combined thus eliminating the need for venous phase and excretory phase scanning."
Combined Vascular-Excretory Phase MDCT Angiography in the Preoperative Evaluation of Renal Donors
Zamboni GA et al.
AJR 2010; 194:145-150"Split-bolus contrast injection and combined vascular phase scanning are adequate for studying potential renal donors and result in a marked decrease in multiphase scanning, and thus radiation dose."
Combined Vascular-Excretory Phase MDCT Angiography in the Preoperative Evaluation of Renal Donors
Zamboni GA et al.
AJR 2010; 194:145-150- "Laparoscopic donor nephrectomy has become the accepted method of harvesting the kidney at many institutions because of multiple advantages over open donor nephrectomy. Spiral computed tomographic (CT) angiography provides accurate information of renal vascular anatomy and has become an accepted method of preoperative evaluation of potential laparoscopic renal donors."
MDCT Angiography of Living Laparoscopic Renal Donors Kawamoto S, Fishman EK
Abdom Imaging 2006.
- "Multiple renal arteries were seen in 26% of kidneys. Early branching of the main renal artery was seen in 12% of kidneys."
Assessment of 100 Live Potential renal Donors for Lapatoscopic Nephrectomy with Multidetector Row Helical CT
Holden A et al.
Radiology 2005; 237:973-980
- "In conclusion, multidetector row CT enables highly accurate assessment of the renal anatomy in living donor candidates."
Assessment of 100 Live Potential renal Donors for Lapatoscopic Nephrectomy with Multidetector Row Helical CT
Holden A et al.
Radiology 2005; 237:973-980
- "Multidetector row CT can help assess well the renal vasculature and the urinary tract of living renal donors."
Living Donor Kidneys: Usefulness of Multi-Detector Row CT for Comprehensive Evaluation
Kim JK et al.
Radiology 2003; 229:869-876
- "Detection rate of CT angiography was 98% for arteries and 98% for veins."
Living Donor Kidneys: Usefulness of Multi-Detector Row CT (4 row) for Comprehensive Evaluation
Kim JK et al.
Radiology 2003; 229:869-876