|
-- OR -- |
|
- Adenomas are the most common type of adrenal tumor, representing 90% of all adrenal incidentalomas, with the majority being metabolically inactive. However, 7.1% of benign adenomas can secrete metabolically active substances, including aldosterone (1%) and glucocorticoids (6%), leading to Conn’s syndrome and Cushing’s syndrome, respectively. Exceedingly rare is the ability of these adenomas to secrete sex hormones. The physiologic activity of these hormones and their associated medical syndromes are covered elsewhere in this issue, but the evaluation for secretion of metabolically active substances places tumors with such capability under the purview of this rare tumor article. Tumors that do not initially possess the ability to secrete metabolic substances rarely gain the ability to do so. The rate of transformation to metabolically active adenoma has been documented at 1.7% but is exceedingly rare.
Rare Adrenal Tumors and Adrenal Metastasis
Steven Leonard, BSa, Marc C. Smaldone, MD, MSHPb
Urol Clin N Am - (2025) (in press) - “Classic external symptoms of Cushing syndrome include central obesity, abdominal striae, buffalo hump, and moon facies. Laboratory findings may also include dyslipidemia, hyperglycemia, and hypertension. Laboratory evaluation for the diagnosis of Cushing syndrome involves either measurement of 24-hour urinary-free cortisol level or low-dose dexamethasone suppression testing. Any abnormal result warrants referral to an endocrine specialist for definitive diagnosis. In evaluation of the origin of Cushing syndrome, the lowdose dexamethasone suppression test can be useful.”
Rare Adrenal Tumors and Adrenal Metastasis
Steven Leonard, BSa, Marc C. Smaldone, MD, MSHPb
Urol Clin N Am - (2025) (in press) - “As with adenomas, myelolipomas are typically diagnosed with cross-sectional imaging, and CT scan offers excellent value in the characterization of the lesion. Like adenomas, these lesions are well defined with smooth borders. However, myelolipomas contain elements of myeloid tissue among their fatty components, and on CT scan, these areas display greater attenuation. The myeloid tissue will further enhance with contrast. Some myelolipomas display calcification or areas of hemorrhage. MRI can also be used to further characterize myelolipomas. If fat is visualized on MRI, then myelolipoma diagnosis is highly likely, although definitive diagnosis still requires tissue sampling.”
Rare Adrenal Tumors and Adrenal Metastasis
Steven Leonard, BSa, Marc C. Smaldone, MD, MSHPb
Urol Clin N Am - (2025) (in press) - “Ganglioneuromas are exceedingly rare neoplasms that may arise from the adrenal gland in 40% of cases. However, they may also develop anywhere along the sympathetic chain, including the cervical (5%), thoracic (15%), abdominal (25%), and pelvic (5%) chain. These tumors are most common in children, but when discovered in adults, it is usually incidentally in the fourth or fifth decade of life. These neoplasms are benign and can grow quite large, but most are asymptomatic. 3If symptoms exist, diarrhea or hypertension may be the presenting symptom secondary to vasoactive intestinal peptide or catecholamine secretion in a minority of ganglioneuromas. These neoplasms have also been shown to encase vessels without impingement or invasion of the lumen, and such cases pose a challenge to surgical resection.”
Rare Adrenal Tumors and Adrenal Metastasis
Steven Leonard, BSa, Marc C. Smaldone, MD, MSHPb
Urol Clin N Am - (2025) (in press)
- “Atypical adrenal adenomas include those that are lipid poor; contain macroscopic fat, hemorrhage, and/or iron; are heterogeneous and/or large; and demonstrate growth. Heterogeneous adrenal adenomas may mimic ACC, metastasis, or pheochromocytoma, particularly when they are 4 cm or larger, whereas smaller versions of ACC, metastasis, and pheochromocytoma and those with washout greater than 60% may mimic adenoma. Because of its nonenhanced CT attenuation of less than or equal to 10 HU, a lipid-rich adrenal adenoma may be mimicked by a benign adrenal cyst, or it may be mimicked by a tumor with central cystic and/or necrotic change such as ACC, pheochromocytoma, or metastasis.”
Adrenal Neoplasms: Lessons from Adrenal Multidisciplinary Tumor Boards
Ryan Chung et al.
RadioGraphics 2023; 43(7):e220191 July 2023 - “Adrenal adenoma is the most common benign adrenal tumor that arises from the cortex, whereas adrenocortical carcinoma (ACC) is a rare malignant tumor of the cortex. Adrenal cyst and myelolipoma are other benign adrenal lesions and are characterized by their fluid and fat content, respectively. Pheochromocytoma is a rare neuroendocrine tumor of the adrenal medulla. Metastases to the adrenal glands are the most common malignant adrenal tumors. While many of these masses have classic imaging appearances, considerable overlap exists between benign and malignant lesions and can pose a diagnostic challenge.”
Adrenal Neoplasms: Lessons from Adrenal Multidisciplinary Tumor Boards
Ryan Chung et al.
RadioGraphics 2023; 43(7):e220191 July 2023 - “More recent data have shown that these values are not as specific for adenoma as previously believed, since other adrenal tumors such as pheochromocytoma, hypervascular metastases, and ACC also can meet these washout thresholds. Other features such as mass size, heterogeneity, and clinical context (eg, history of hypervascular malignancy or suspicion for pheochromocytoma) must be taken into account when using washout CT.”
Adrenal Neoplasms: Lessons from Adrenal Multidisciplinary Tumor Boards
Ryan Chung et al.
RadioGraphics 2023; 43(7):e220191 July 2023 - “In a relatively recent study, nearly one-third of adenomas grew over time, all at a rate of less than 3 mm per year, as compared with all malignant nodules, which grew at a rate of greater than 5 mm per year. A growth rate of less than 3 mm per year distinguished the adenomas from the malignant nodules with a sensitivity and specificity of 100%.”
Adrenal Neoplasms: Lessons from Adrenal Multidisciplinary Tumor Boards
Ryan Chung et al.
RadioGraphics 2023; 43(7):e220191 July 2023 - “Because the attenuation of simple fluid is less than or equal to 10 HU, a homogeneous unilocular cystic adrenal lesion can mimic adenoma at nonenhanced CT. Owing to their central hypoattenuation, cysts and pseudocysts may also mimic pheochromocytomas with cystic and/or necrotic change. A key feature of an adrenal cyst is its lack of enhancement.”
Adrenal Neoplasms: Lessons from Adrenal Multidisciplinary Tumor Boards
Ryan Chung et al.
RadioGraphics 2023; 43(7):e220191 July 2023
- "In contrast to the approach taken by the ACR, the American Association of Clinical Endocrinologists and American Association of Endocrine Surgeons has taken a more conservative approach and recommend imaging evaluation 3 to 6 months after the initial diagnosis, and then annually for 1 to 2 years for all nodules less than 4 cm, even those with benign characteristics. The European Society of Endocrinology and the European Network for the Study of Adrenal Tumors has taken a simpler approach and recommend no further follow-up imaging for nodules less than 4 cm with a nonenhanced attenuation of less than 10 HU (ie, those that can be diagnosed as lipid-rich adenomas).”
Incidental Adrenal Nodules
Daniel I. Glazer, Michael T. Corwin, William W. Mayo-Smith
Radiol Clin N Am 59 (2021) 591–601 - “Incidentally detected adrenal nodules are com- mon, and prevalence increases with patient age. Although almost all are benign, it is important for the radiologist to be able to accurately determine which nodules require further testing and which are safely left alone. The most recent ACR inci- dental adrenal White Paper provides a structured algorithm based on expert consensus for manage- ment of incidental adrenal nodules. If further diag- nostic testing is indicated, adrenal CT is the most appropriate test in patients for all nodules less than 4 cm regardless of cancer history. In addition to imaging, biochemical testing and endocrinology referral may be warranted to exclude a functioning mass (which should then be resected regardless of imaging features)."
Incidental Adrenal Nodules
Daniel I. Glazer, Michael T. Corwin, William W. Mayo-Smith
Radiol Clin N Am 59 (2021) 591–601
- Bilateral Adrenal Masses: Benign
- Adenoma
- Myelolipoma
- Infection (TB)
- Hematoma - Bilateral Adrenal Masses: Non-Mass Like
- Adrenal hyperplasia
- Adrenal atrophy
- Adrenal calcifications (Wolman’s Disease)
- Intense enhancement (hypoperfusion syndrome)
- Adrenal Adenoma: CT Findings
• typically well-defined
• often homogeneous in attenuation (87% homogeneous on precontrast images, 58% homogeneous on • postcontrast images)
• average diameters of 2–2.5 cm
• Adenomas can be over 4 cm in size - Adrenal Adenoma: CT Findings
• The precontrast attenuation varies accord- ing to the presence or absence of lipid, with mean attenuation in the range of −2 to 16 HU in lipid-rich adenomas and higher attenuation (20–25 HU) seen • in the setting of lipid-poor adenomas
adenomas typically demonstrate rapid washout, which is defined as an APW of more than 60% and an • RPW of more than 40% on delayed images - Adrenal Adenoma: CT Findings
Combined unenhanced and contrast-enhanced CT can be used to identify lipid-poor adenomas (less than 10 HU) using washout calculations.This technique raises both the sensitivity and specificity of CT to 96 percent for adrenal adenoma diagnosis.
- “The characteristic CT findings of adrenal adenoma with the maximal diameter greater than 5 cm include bulky, well-circumscribed, rounded or ovoid masses, heterogeneous attenuation with low-attenuation foci on non-enhanced CT images and heterogeneous enhancement after contrast administration. The differential diagnosis between such tumor and adrenal cortical carcinoma by CT examination is relatively difficult, such findings as recurrence, metastasis and venous tumor emboli may be of some significance.”
Adrenal cortical adenoma with the maximal diameter greater than 5 cm: can they be differentiated from adrenal cortical carcinoma by CT?
Tian L et al.
Int J Clin Exp Med. 2014 Oct 15;7(10):3136-43. - “The maximal diameter of the 14 masses of adenoma ranged from 5.5 cm to 20 cm (mean, 10 cm). One mass showed lobulated, the rest 13 masses showed rounded or ovoid. Eleven and 3 masses appeared well-circumscribed and ill-circumscribed, respectively. All of 14 masses presented heterogeneous density on non-enhanced CT images with patchy low-attenuation foci or stippled calcification. All of 14 masses revealed moderately to markedly heterogeneous enhancement after contrast administration.”
Adrenal cortical adenoma with the maximal diameter greater than 5 cm: can they be differentiated from adrenal cortical carcinoma by CT?
Tian L et al.
Int J Clin Exp Med. 2014 Oct 15;7(10):3136-43. - “ None of 14 masses developed local invasion and distant metastasis. Except for recurrence, metastasis and venous tumor emboli which only occurred in the cases of adrenal carcinoma, no definite computed tomographic features could be found that enabled the identification of adenomas with the maximal diameter greater than 5 cm with adrenal carcinomas.”
Adrenal cortical adenoma with the maximal diameter greater than 5 cm: can they be differentiated from adrenal cortical carcinoma by CT?
Tian L et al.
Int J Clin Exp Med. 2014 Oct 15;7(10):3136-43. 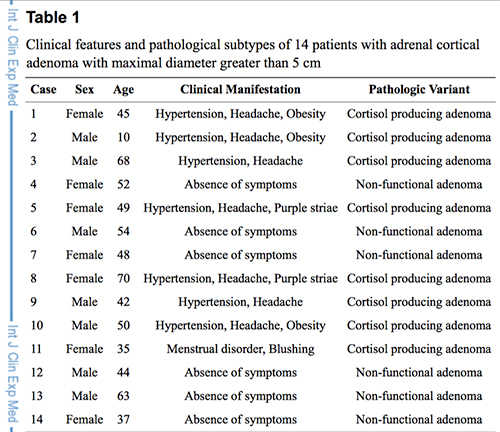

- “ MRI is equivalent to CT for characterizing adenomas measuring 20 HU or less on unenhanced CT. However, MRI is inferior to CT for adenomas measuring more than 20 HU because of decreased MR sensitivity.”
Characterization of Lipid Poor Adrenal Adenoma: Chemical Shift MRI and Washout CT
Seo JM et al.
AJR 2014;202:1043-1050 - “ The sensitivities for adenomas measuring 20 HU or less on unenhanced CT were 100% in both MRI and CT, whereas those measuring more than 20 HU were 64% (16/25) and 100% (25/25) in MRI and CT , respectively.”
Characterization of Lipid Poor Adrenal Adenoma: Chemical Shift MRI and Washout CT
Seo JM et al.
AJR 2014;202:1043-1050 - “ A cutoff value of 10 HU provides sensitivity of 71% and specificity of 98%. Therefore, approximately 70% of adenomas can be correctly diagnosed on unenhanced CT without the use of IV contrast material. The remaining 30% of adenomas, however, require another imaging modality for characterization.”
Characterization of Lipid Poor Adrenal Adenoma: Chemical Shift MRI and Washout CT
Seo JM et al.
AJR 2014;202:1043-1050
- Adrenal Insufficiency
-Bilateral hemorrhage à adrenal insufficiency
-Nonspecific symptoms
-Fatigue, weakness, muscle/joint pain
-Abdominal pain, vomiting, diarrhea
-Depression, behavioral changes
-Hypotension - Adenoma with Hemorrhage
-Rarely an adenoma can hemorrhage
-Usually anticoagulated patient
-Heterogeneous
-Regions of high attenuation "In clinical practice therefore, 10 HU is the most widely used threshold value for the diagnosis of lipid-rich adrenal adenoma."
Adrenal Imaging
Blake MA et al.
AJR 2010; 194:1450-1460"In conclusion the 10 minute delayed adrenal enhancement washout tests have reduced sensitivity for the detection of adenomas compared with results from prior studies, and the test sensitivity appears to be clinically suboptimal. This finding might be explained by insufficient time for the intravenous contrast material to wash out from benign lesions."
Incidental Adrenal Lesions: Accuracy of Characterization with Contrast-enhanced Washout Multidetector CT—10-minute Delayed Imaging Protocol Revisited in a Large Patient Cohort
Sangwaiya MJ et al.
Radiology 2010; 256:504-510"Ten minute delayed multidetector CT adrenal washout tests have reduced accuracy compared with results from prior studies; overall test accuracy at 40% threshold was 77.7% according to our test results."
Incidental Adrenal Lesions: Accuracy of Characterization with Contrast-enhanced Washout Multidetector CT—10-minute Delayed Imaging Protocol Revisited in a Large Patient Cohort
Sangwaiya MJ et al.
Radiology 2010; 256:504-510- "The 10-minute delayed adrenal enhancement washout test has reduced sensitivity for the characterization of adrenal adenomas compared with results from prior studies."
Incidental Adrenal Lesions: Accuracy of Characterization with Contrast-enhanced Washout Multidetector CT—10-minute Delayed Imaging Protocol Revisited in a Large Patient Cohort
Sangwaiya MJ et al.
Radiology 2010; 256:504-510 "The high diagnostic accuracy leads to a decrease in the number of patients with an indeterminate adrenal mass, which requires the other diagnostic methods including MR imaging, radionuclide imaging, and adrenal biopsy."
Distinguishing Adrenal Adenomas from Nonadenomas: Combined Use of Diagnostic Parameters of Unenhanced and Short 5-minute Dynamic Enhanced CT Protocol
Kamiyama T et al
Radiology 2009; 250:474-481- Adrenal: Adrenal Adenoma: CT Criteria
- Attenuation of less than or equal to 10HU on unenhanced CT
- Absolute contrast washout of greater than or equal to 52 HU at 10 minutes or 60% at 15 minutes (100 ml injection of Omnipaque-350 at 3ml/sec)