|
-- OR -- |
|
- Adrenal Adenoma: CT Findings
• typically well-defined
• often homogeneous in attenuation (87% homogeneous on precontrast images, 58% homogeneous on • postcontrast images)
• average diameters of 2–2.5 cm
• Adenomas can be over 4 cm in size - Adrenal Adenoma: CT Findings
• The precontrast attenuation varies accord- ing to the presence or absence of lipid, with mean attenuation in the range of −2 to 16 HU in lipid-rich adenomas and higher attenuation (20–25 HU) seen • in the setting of lipid-poor adenomas
adenomas typically demonstrate rapid washout, which is defined as an APW of more than 60% and an • RPW of more than 40% on delayed images - Adrenal Adenoma: CT Findings
Combined unenhanced and contrast-enhanced CT can be used to identify lipid-poor adenomas (less than 10 HU) using washout calculations.This technique raises both the sensitivity and specificity of CT to 96 percent for adrenal adenoma diagnosis.
- Cushing Syndrome: Clinical Findings
• Central obesity fat accumulation in trunk, supraclavicular, and dorsocervical regions (i.e., buffalo hump), and around face (i.e., moon facies); mediastinal lipomatosis
• Skin thinning and friability
• Osteoporosis
• Impaired immune system
• Proximal muscle weakness - Cushing Syndrome due to
Endogenous Cushing Syndrome
• Administration of glucocorticoids (iatrogenic CS)
• Administration of synthetic ACTH
• Administration of medroxyprogesterone
• Cushing Syndrome due to ACTH-Dependent CS (80% of Endogenous Causes)
• Pituitary-tumor producing ACTH (Cushing disease) (80%)
• Ectopic ACTH-producing tumor (20%)
• Corticotropin-releasing hormone producing tumor (< 1%) - Cushing Syndrome due to
ACTH-Independent CS (20% of Endogenous Causes)
• Adrenal lesions producing cortisol autonomously
• Adrenal adenoma (60%)
• Adrenocortical carcinoma (40%)
• Primary pigmented nodular adrenal disease (< 1%)
• ACTH-independent macronodular adrenocortical hyperplasia (< 1%) - Cushings Syndrome: CT Findings
• Adrenal adenoma (60%)
• Adrenocortical carcinoma (40%)
• Primary pigmented nodular adrenal disease (< 1%)
• ACTH-independent macronodular adrenocortical hyperplasia (< 1%) - Cushings Syndrome: CT Findings
Adrenocortical carcinoma—ACCs are rare often-aggressive tumors and account for approximately 40% of adrenal causes of CS. ACCs have an estimated annual incidence of two cases per million people with an estimated 5-year overall survival rate of 15–44%. ACC tends to occur in the fourth or fifth decades of life and only extremely rarely in children - Cushings Syndrome: CT Findings
Adrenal Carcinoma accounts for approximately 40% of adrenal causes of CS and usually appears as a unilateral large (mean size, 9 cm; range, 2–25 cm) heterogeneously enhancing soft-tissue mass, frequently with intratumoral necrosis or hemorrhage, with microscopic or coarse calci cations present in 30% of cases.
- Primary Aldosteronomas: Facts
• First described by Conn in 1955
• Age at presentation is between 30-50 years and and more common in woman
• Characterized by hypertension, suppressed plasma renin activity and increased aldosterone secretion
• Two thirds of patients have bilateral idiopathic hyperaldosteronism and approximately one third have aldosterone producing adenomas - “Primary aldosteronism is defined as the inappropriate autonomous hypersecretion of aldosterone in the absence of activation of the renin-angiotensin-aldosterone axis. Primary aldosteronism is the most common cause of secondary hypertension and is estimated to be responsible for 5%–20% of all cases of hypertension.”
Role of Radiology in the Management of Primary Aldosteronism Patel SM et al. RadioGraphics 2007; 27:1145–1157 - “Primary aldostenonism, or Conn’s
cause of hypertension. Approximately
have a benign aldosterone-secreting
of the remaining patients have bilateral adrenal hyperplasia. Adrenal carcinoma has been reported as a cause of Conn’s syndrome, but this is rare.”
CT in the Diagnosis of Primary Aldosteronism: Sensitivity in 29 Patients Dunnick NR et al. AJR 1 993;160:321-324 - “APAs are benign adrenocortical neoplasms associated with pathologic aldosterone excess. At gross examination, they are usually yellow, round or oval, and typically less than 2 cm in size, with a significant proportion less than 1 cm. APAs can occur in any age group but are often found in younger patients ( 40 years old).”
Role of Radiology in the Management of Primary Aldosteronism Patel SM et al. RadioGraphics 2007; 27:1145–1157 - “If an adrenal nodule or mass is seen in one adrenal gland but the contralateral gland appears normal, surgery should be considered for the resection of an APA. In older patients, however, owing to the higher prevalence of bilateral (nodular) hyperplasia, the clinician may prefer to use AVS prior to surgery to confirm the diagnosis of an APA.”
Role of Radiology in the Management of Pri- mary Aldosteronism Patel SM et al. RadioGraphics 2007; 27:1145–1157 - Aldosteronomas: CT Appearance
• Can be either due to aldosterone-producing adenoma (APA) or bilateral adrenal hyperplasia (BAH)
• aldosterone-producing adenoma (APA) are usually unilateral and 2cm or less in size
• aldosterone-producing adenoma (APA) can be bilateral and the site of the tumor may require venous sampling - Primary Aldosteronomas: CT Findings
Usually unilateral but may be bilateral
• Mean diameter is 1.5 to 2.0 cm
• No significant enhancement
• Sensitivity for localizing a Primary Aldosteronomas with CT is 82-90%
• Key is thin section CT on current state of the art scanner - “ A 100% specificity for diagnosing bilateral adrenal hyperplasia was achieved with a mean adrenal limb width greater than or equal to 5 mm and 100% sensitivity with a mean width greater than 3 mm.”
Role of Radiology in the Management of Primary Aldosteronism Patel SM et al. RadioGraphics 2007; 27:1145-1157 - “In the setting of hyperaldosteronism (Conn's syndrome), the absence of an adenoma traditionally suggested adrenal hyperplasia as the cause. With improved CT resolution, gland measurements have proven useful. Lingam et al. revealed that the medial and lateral limbs were significantly larger in hyperplasia. A cutoff of 5 mm was 47% sensitive and 100% specific; using a 3-mm cutoff, sensitivity was 100% and specificity, 54%. In comparison, the absence of an adenoma at imaging was 93.3% sensitive and 84.6% specific.”
Adrenal Imaging with MDCT: Nonneoplastic Disease Johnson PT, Horton KM, Fishman EK AJR 2009;193: 1128-1135 - “Cushing syndrome (CS) is a constellation of clinical signs and symptoms resulting from chronic exposure to excess cortisol, either exogenous or endogenous. Exogenous CS is most commonly caused by administration of glucocorticoids. Endogenous CS is subdivided into two types: adrenocorticotropic hormone (ACTH) dependent and ACTH independent.”
Cushing Syndrome: Diagnostic Workup and Imaging Features, With Clinical and Pathologic Correlation Wagner-Bartak NA et al. AJR 2017; 209:19–32
- Adrenal Metastases: Sites of Origin
• Lung
• Gastric or esophageal cancer
• Hepatic-biliary or pancreatic cancer
• Colon cancer
• Renal cancer
• Breast cancer
• Melanoma
• Sarcoma
• Hematopoietic tumors - “In patients with RCC and HCC who undergo dedicated adrenal CT imaging for known adrenal lesions, the percentage enhancement washout of adrenal metastases is similar to that of lipid-poor adrenal adenomas. Careful imaging follow-up or pathologic tissue confirmation is needed."
Evaluation of adrenal metastases from renal cell carcinoma and hepatocellular carcinoma: Use of Delayed Contrast-enhanced CT Choi YA et al. Radiology 2013; 266:514–520 - “For the workup of adrenal masses in patients with extraadrenal primary RCC or HCC, a careful serial imaging follow-up or tissue con rmation at biopsy or surgery is recommended to exclude the possibility of metastasis."
Evaluation of adrenal metastases from renal cell carcinoma and hepatocellular carcinoma: Use of Delayed Contrast-enhanced CT Choi YA et al. Radiology 2013; 266:514–520 - Adrenal Metastases: CT Findings
• Variable size but often size greater than 4-6 cm
• interval change in size
• irregular shape and necrosis
• invasion of adjacent structures
• Vascularity variable but may be hypervascular - Adrenal Metastases: CT Findings
• Adrenal metastases are commonly bilateral
• Large bilateral metastases are often seen with melanoma
• "collision tumors", in which malignancy occurs in or adjacent to a known pre-existing benign adrenal lesion, such as metastatic disease arising within an adrenal adenoma can occur - “Malignant melanoma is an extremely aggressive form of cancer. Adrenal metastases are found in 50% of cases of malignant melanoma, and are most often clinically and biochemically silent. Clinical presentation varies, and the diagnosis of adrenal metastases is often made incidentally, and frequently years after treatment of the primary lesion. An adrenal mass lesion seen on a CT scan, greater than 5 cm in diameter, with central or irregular areas of necrosis/haemorrhage (and no lipomatous component) is characteristic of a metastasis from malignant melanoma, in the setting of normal gland function. If these features are bilateral, they are pathognomonic. Oval, low-attenuation (on CT) adrenal masses less than 3 cm in diameter should not be considered benign in a patient with any prior history of melanoma.”
Adrenal metastases of malignant melanoma: characteristic computed tomography appearances. Rajaratnam A1, Waugh J. Australas Radiol. 2005 Aug;49(4):325-9.
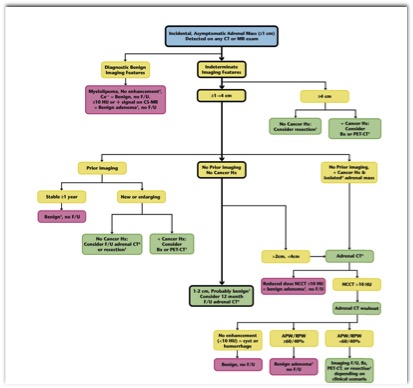
- Flowchart for an adrenal mass
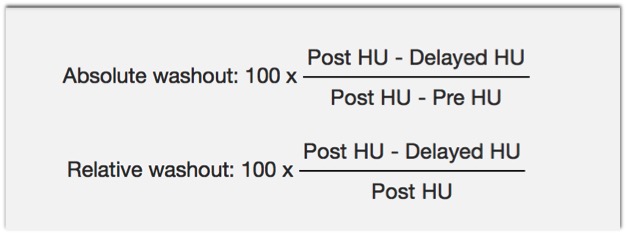
- Adrenal Washout Values
- “ The preferred work-up scheme for the indeterminate adrenal mass includes evaluation with a non-contrast CT. If a lesion is less than 10 HU < 10 on a non-contrast CT, it is a benign lipid-rich adenoma and no further work-up is needed. A lipid-poor adenoma can be differentiated from a metastasis utilizing CT wash-out patterns or MRI.”
Cross-sectional imaging work-up of adrenal masses Korivi BR, Elsayes KM World J Radiol. 2013 Mar 28; 5(3): 88–97 - “ The preferred work-up scheme for the indeterminate adrenal mass includes evaluation with a non-contrast CT. If a lesion is less than 10 HU < 10 on a non-contrast CT, it is a benign lipid-rich adenoma and no further work-up is needed. A lipid-poor adenoma can be differentiated from a metastasis utilizing CT wash-out patterns or MRI.”
Cross-sectional imaging work-up of adrenal masses Korivi BR, Elsayes KM World J Radiol. 2013 Mar 28; 5(3): 88–97. - “ Lipid-poor adenomas have an attenuation of more than 10 non-contrast HU and can be further characterized by their contrast enhancement and wash-out patterns. Only 30% of adenomas are lipid poor, which renders further characterization with contrast necessary. Adenomas tend to rapidly enhance after contrast administration and rapidly wash-out. Malignant lesions and pheochromocytomas also enhance rapidly but tend to exhibit slower wash-out patterns. Two methods have been developed to calculate wash-out patterns: the percentage of absolute contrast enhancement wash-out (ACEW) and the relative contrast enhancement wash-out (RCEW).
Cross-sectional imaging work-up of adrenal masses Korivi BR, Elsayes KM World J Radiol. 2013 Mar 28; 5(3): 88–97. - absolute contrast enhancement wash-out (ACEW)
• If a 15 min delay protocol is used, an ACEW value of 60% or higher has approximately 87% sensitivity and 94% specificity
• Note that ACEW measurements require a non-contrast HU measurement and in everyday practice, this is not always obtained. - relative contrast enhancement wash-out (RCEW).
• the percentage of RCEW can be calculated as: % RCEW = [(contrast-enhanced HU at 60 s - delayed contrast HU)/(contrast-enhanced HU at 60 s)] × 100.
• If a 15 min delay parameter is used, a RCEW of 40% or more has a sensitivity of 96% and specificity of 100% - OBJECTIVE. The purpose of this article is to retrospectively compare the accuracy of MRI and CT in characterizing lipid-poor adrenal adenomas with respect to lesion-attenuation values measured on unenhanced CT.
CONCLUSION. MRI is equivalent to CT for characterizing adenomas measuring 20 HU or less on unenhanced CT. However, MRI is inferior to CT for adenomas measuring more than 20 HU because of decreased MR sensitivity.
Characterization of Lipid-Poor Adrenal Adenoma: Chemical-Shift MRI and Washout CT Seo JM et al. AJR 2014; 202:1043–1050 - “Approximately 30% of adrenal adenomas are lipid-poor and cannot be differentiated from nonadenomas using unenhanced CT alone because these lipid-poor adenomas measure greater than 10 HU. Washout CT characterizes these lipid-poor adenomas with sensitivity of almost 100%.”
Characterization of Lipid-Poor Adrenal Adenoma: Chemical-Shift MRI and Washout CT Seo JM et al. AJR 2014; 202:1043–1050


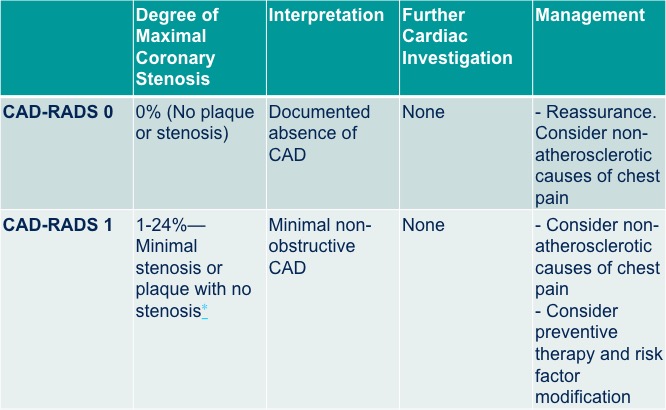
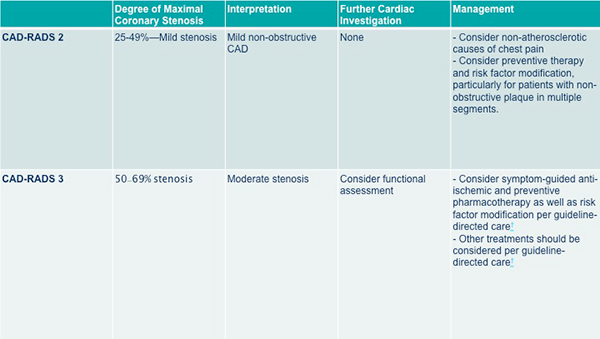
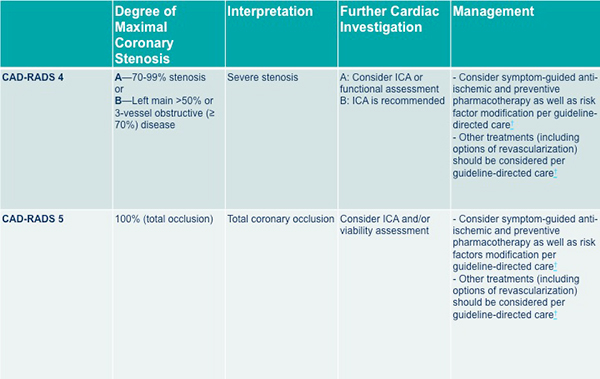
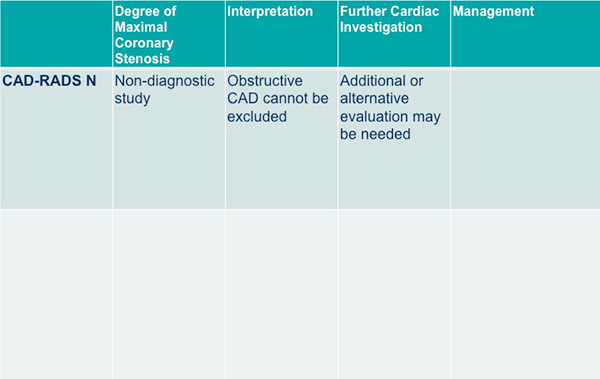
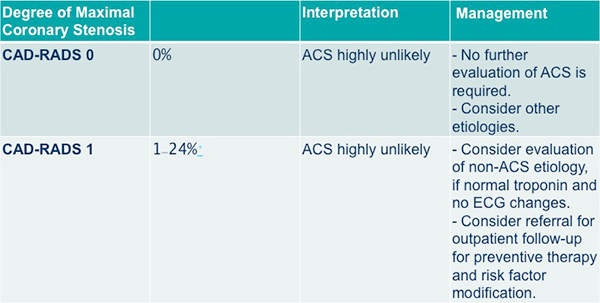
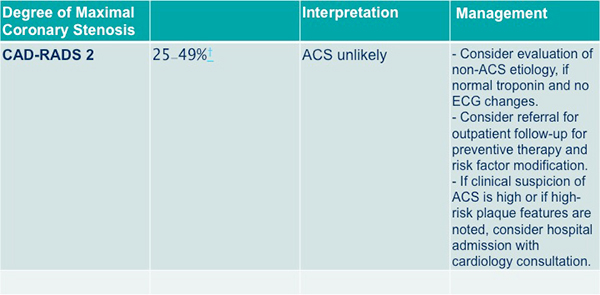
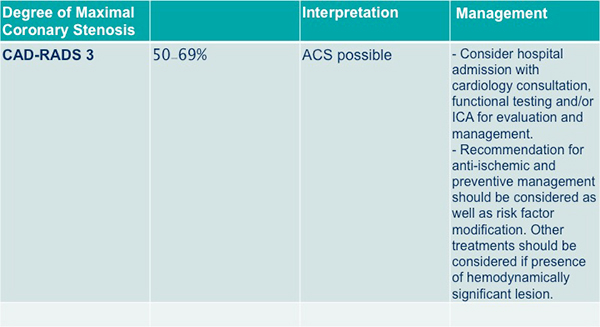
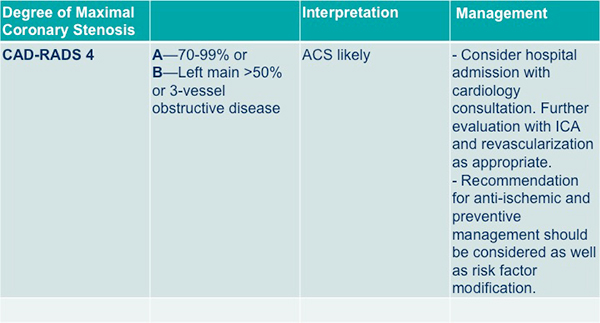
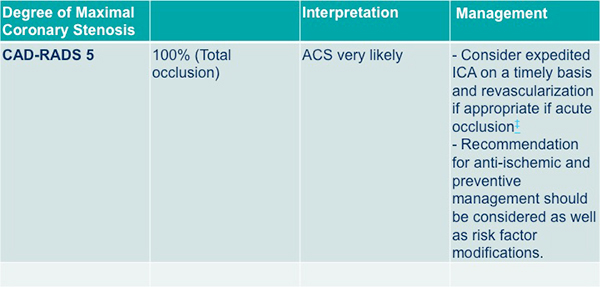
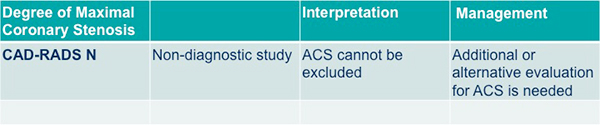
“The intent of CAD-RADS – Coronary Artery Disease Reporting and Data System is to create a standardized method to communicate findings of coronary CT angiography (coronary CTA) in order to facilitate decision-making regarding further patient management.”
CAD-RADS™: Coronary Artery Disease - Reporting and Data System: An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Radiology (ACR) and the North American Society for Cardiovascular Imaging (NASCI). Endorsed by the American College of Cardiology. Cury RC et al. J Am Coll Radiol. 2016 Dec;13(12 Pt A):1458-1466.“The suggested CAD-RADS classification is applied on a per-patient basis and represents the highest-grade coronary artery lesion documented by coronary CTA. It ranges from CAD-RADS 0 (Zero) for the complete absence of stenosis and plaque to CAD-RADS 5 for the presence of at least one totally occluded coronary artery and should always be interpreted in conjunction with the impression found in the report. Specific recommendations are provided for further management of patients with stable or acute chest pain based on the CAD-RADS classification.”
CAD-RADS™: Coronary Artery Disease - Reporting and Data System: An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Radiology (ACR) and the North American Society for Cardiovascular Imaging (NASCI). Endorsed by the American College of Cardiology. Cury RC et al. J Am Coll Radiol. 2016 Dec;13(12 Pt A):1458-1466.“The main goal of CAD-RADS is to standardize reporting of coronary CTA results and to facilitate communication of test results to referring physicians along with suggestions for subsequent patient management. In addition, CAD-RADS will provide a framework of standardization that may benefit education, research, peer-review and quality assurance with the potential to ultimately result in improved quality of care.”
CAD-RADS™: Coronary Artery Disease - Reporting and Data System: An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Radiology (ACR) and the North American Society for Cardiovascular Imaging (NASCI). Endorsed by the American College of Cardiology. Cury RC et al. J Am Coll Radiol. 2016 Dec;13(12 Pt A):1458-1466.Reporting Standards
BI-RADS (Breast Imaging with standardized reporting of screening mammograms )
LI-RADS™ (Liver Imaging Reporting and Data System) for standardization reporting in patients with chronic liver disease.
Lung-RADS™ (Lung CT Screening Reporting and Data System) for standardization reporting of high-risk smokers undergoing CT lung screening.
PI-RADS™ (Prostate Imaging Reporting and Data System) for multi-parametric MR imaging in the context of prostate cancer.“The goal of CAD-RADS, through standardization of report terminology for coronary CTA, is to improve communication between interpreting and referring physicians, facilitate research, and offer mechanisms to contribute to peer review and quality assurance, ultimately resulting in improvements to quality of care. Importantly, CAD-RADS does not substitute the impression section provided by the reading physician and should always be interpreted in conjunction with the more individual and patient-specific information found in the report.”
CAD-RADS™: Coronary Artery Disease - Reporting and Data System: An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Radiology (ACR) and the North American Society for Cardiovascular Imaging (NASCI). Endorsed by the American College of Cardiology. Cury RC et J Am Coll Radiol. 2016 Dec;13(12 Pt A):1458-1466.“The main clinical benefit of coronary CTA is derived from its high sensitivity and negative predictive value. The positive predictive value of coronary CTA is lower, and especially intermediate lesions may be overestimated regarding their relevance. Many patients with previously known CAD will include lesions that fall into this category, so that coronary CTA will need to be complemented by further tests.”
CAD-RADS™: Coronary Artery Disease - Reporting and Data System: An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Radiology (ACR) and the North American Society for Cardiovascular Imaging (NASCI). Endorsed by the American College of Cardiology. Cury RC et J Am Coll Radiol. 2016 Dec;13(12 Pt A):1458-1466.“The use of coronary CTA to assess patients with stable chest pain in the outpatient setting or acute chest pain presenting to the Emergency Department has been validated in various clinical trials. Major guidelines are incorporating the use of coronary CT angiography as appropriate for assessing low to intermediate risk patients presenting with chest pain. Decreasing the variation in reporting is one aspect that will contribute to wider dissemination in clinical practice, minimize error and to ultimately improve patient outcome. The main goal of the CAD-RADS classification system is to propose a reporting structure that provides consistent categories for final assessment, along with suggestions for further management.”
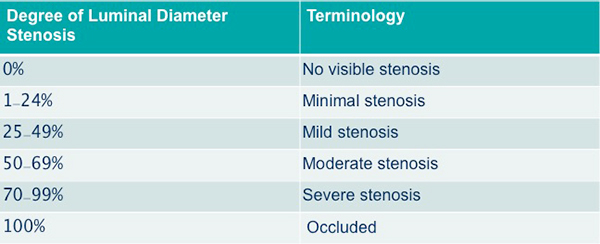
CAD-RADS™: Coronary Artery Disease - Reporting and Data System: An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Radiology (ACR) and the North American Society for Cardiovascular Imaging (NASCI). Endorsed by the American College of Cardiology. Cury RC et J Am Coll Radiol. 2016 Dec;13(12 Pt A):1458-1466.SCCT Grading for Coronary Artery Stenosis
CAD-RADS Reporting and Data System for patients presenting with stable chest pain
CAD-RADS Reporting and Data System for patients presenting with stable chest pain
CAD-RADS Reporting and Data System for patients presenting with stable chest pain
CAD-RADS Reporting and Data System for patients presenting with stable chest pain
Acute chest pain, negative first troponin, negative or non-diagnostic electrocardiogram and low to intermediate risk (TIMI risk score < 4)
Acute chest pain, negative first troponin, negative or non-diagnostic electrocardiogram and low to intermediate risk (TIMI risk score < 4)
Acute chest pain, negative first troponin, negative or non-diagnostic electrocardiogram and low to intermediate risk (TIMI risk score < 4)
Acute chest pain, negative first troponin, negative or non-diagnostic electrocardiogram and low to intermediate risk (TIMI risk score < 4)
Acute chest pain, negative first troponin, negative or non-diagnostic electrocardiogram and low to intermediate risk (TIMI risk score < 4)
Acute chest pain, negative first troponin, negative or non-diagnostic electrocardiogram and low to intermediate risk (TIMI risk score < 4)











- “Having small amounts of good-quality data is certainly better than having no data at all. Data augmentation can be used to artificially enlarge the size of a small dataset. The idea is to apply random transformations to the data that do not change the appropriateness of the label assignments. Possible random transformations that can be applied to images include ipping, rotation, translation, zooming, skewing, and elastic deformation. Hence, with data augmentation, image variants from an original dataset are created to enlarge the size of a training dataset of images presented to the deep learning models.”
Deep Learning: A Primer for Radiologists Chartrand G et al. RadioGraphics 2017; 37:2113–2131 - “Even in computer vision, where CNNs have become a dominant method, there are important limitations for deep learning.The most prominent limitation is that deep learning is an intensely data-hungry technology; learning weights for a large network from scratch requires a very large number of labeled examples to achieve accurate classification. However, unlike traditional approaches to computer vision and machine learning, which do not scale well with dataset size, deep learning does scale well with large datasets.”
Deep Learning: A Primer for Radiologists Chartrand G et al. RadioGraphics 2017; 37:2113–2131 - “As a result, building large labeled public medical image datasets is an important step for further progress in applying deep learning to radiology. Barriers to this effort include privacy concerns for clinical images, as well as the costs and difficulties of obtaining accurate ground-truth labels from multiple experts or pathology diagnoses. Nevertheless, several efforts are under way to create large datasets of labeled medical images, such as the Cancer Imaging Archive.”
Deep Learning: A Primer for Radiologists Chartrand G et al. RadioGraphics 2017; 37:2113–2131 - “The role of deep learning and its application to the practice of radiology must still be defined. Deep learning systems may be conceived as a new form of diagnostic test with various clinical usage scenarios . A triage approach would run these automated image analysis systems in the background to detect life-threatening conditions or search through large amounts of clinical, genomic, or imaging data. A replacement approach would use these systems for generating gure captions or even fully automated interpretation of imaging examinations. An add-on approach would support the radiologist by performing time- consuming tasks such as lesion segmentation to assess total tumor burden.”
Deep Learning: A Primer for Radiologists Chartrand G et al. RadioGraphics 2017; 37:2113–2131
“The most frequently encountered pancreatic cysts include IPMN, serous cystadenoma (SCA), mucinous cystic neoplasm with ovarian stroma (MCN), solid pseudopapillary epithelial neoplasm, cystic pancreatic neuroendocrine tumor (cPNET), and pseudocyst. Rare cysts include true epithelial cyst, lymphoepithelial cyst, and mucinous non-neoplastic cyst. IPMN is further subdivided into branch duct (BD), main duct, and combined forms.”
Management of Incidental Pancreatic Cysts: A White Paper of the ACR Incidental Findings Committee. Megibow AJ et al. J Am Coll Radiol. 2017 Jul;14(7):911-923.“Malignancy rates in IPMN are reported as 12%-47% for BD-IPMN, whereas combined form and main duct forms have essentially identical malignancy rates of 38%-65% and 38%-68%, respectively.”
Management of Incidental Pancreatic Cysts: A White Paper of the ACR Incidental Findings Committee. Megibow AJ et al. J Am Coll Radiol. 2017 Jul;14(7):911-923.“Most diagnostic uncertainty is centered on pancreatic cysts <2.5 cm. Helpful queries include the following: (1) Is the cyst mucinous? (2) If mucinous, what is its relation to the main pancreatic duct (MPD)? and (3) If mucinous, are mural nodules present? Several studies suggest that referring physicians are comfortable with imaging surveillance for small BD-IPMN without mural nodules which is supported by pathology studies confirming a low rate of malignant transformation.”
Management of Incidental Pancreatic Cysts: A White Paper of the ACR Incidental Findings Committee. Megibow AJ et al. J Am Coll Radiol. 2017 Jul;14(7):911-923.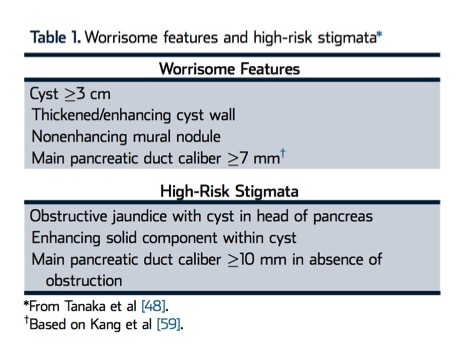
Management of Incidental Pancreatic Cysts: A White Paper of the ACR Incidental Findings Committee. Megibow AJ et al. J Am Coll Radiol. 2017 Jul;14(7):911-923.
Categories
<1.5 cm incidental pancreatic cyst
1.5-2.5 cm incidental pancreatic cyst with MPD communication
1.5-2.5 cm incidental pancreatic cyst without MPD communication or can not be determined
>2.5 cm incidental pancreatic cyst
Incidental pancreatic cyst in patient >80 years oldHow long do you need to follow these patients?
For most patients, we advocate 9- to 10-year follow- up, terminating at the age of 80 years For patients who are <65 years old at the time of initial cyst detection, a follow-up terminating at age 80 will exceed the 9- to 10-year length, but may be prudent ;such decisions regarding additional follow-up should be determined at the individual patient level.
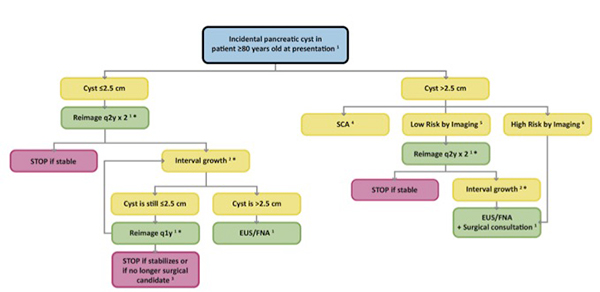
Management of Incidental Pancreatic Cysts: A White Paper of the ACR Incidental Findings Committee. Megibow AJ et al. J Am Coll Radiol. 2017 Jul;14(7):911-923.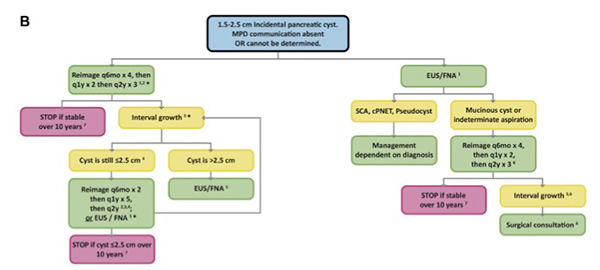
Management of Incidental Pancreatic Cysts: A White Paper of the ACR Incidental Findings Committee. Megibow AJ et al. J Am Coll Radiol. 2017 Jul;14(7):911-923.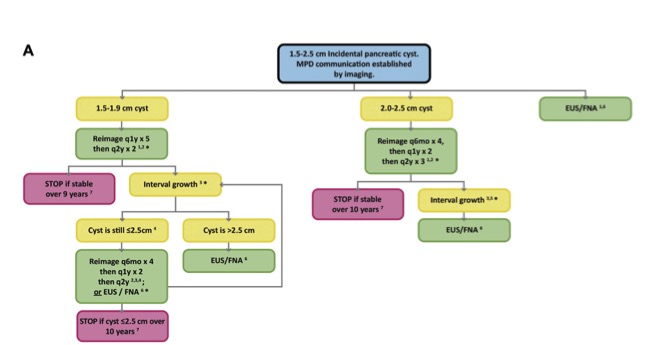
Management of Incidental Pancreatic Cysts: A White Paper of the ACR Incidental Findings Committee. Megibow AJ et al. J Am Coll Radiol. 2017 Jul;14(7):911-923.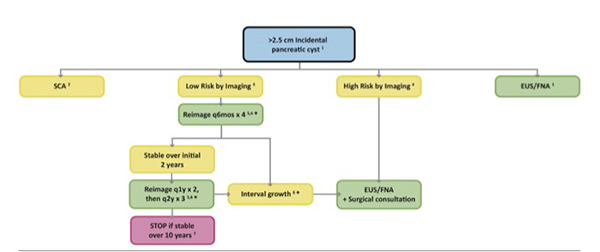
Management of Incidental Pancreatic Cysts: A White Paper of the ACR Incidental Findings Committee. Megibow AJ et al. J Am Coll Radiol. 2017 Jul;14(7):911-923.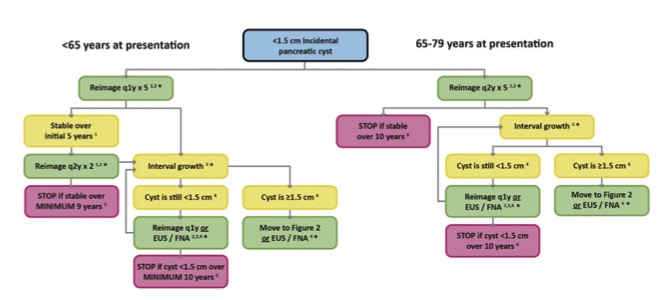
Management of Incidental Pancreatic Cysts: A White Paper of the ACR Incidental Findings Committee. Megibow AJ et al. J Am Coll Radiol. 2017 Jul;14(7):911-923.“The natural history of incidental pancreatic cysts remains uncertain, and our recommendations cannot be simple or entirely definitive. Since 2010, several multi-institutional and specialty society consensus papers, meta-analyses, and large-scale observational studies have appeared but the quality of evidence has been characterized as poor or inconclusive, and conclusions remain controversial.”
Management of Incidental Pancreatic Cysts: A White Paper of the ACR Incidental Findings Committee. Megibow AJ et al. J Am Coll Radiol. 2017 Jul;14(7):911-923.The following six elements must be reported when an incidental pancreatic cyst is detected on a CT or MRI study:
- Cyst morphology, location
- Cyst size
- Possible communication with MPD
- Presence of “worrisome features” and/or “high-risk
- stigmata”
- Growth on follow-up examination
- MultiplicityFive Common Principles of our Algorithm
(1) All incidental cysts should be presumed mucinous, unless the cyst has definitive features of an alternative histology (eg, SCA) or has been proven by aspiration not to be mucinous. Such presumed mucinous cysts should be followed or considered for surgery. We generally recommend 9- to 10-year follow-up with varying schedules, based on initial size. If a cyst grows, the frequency of follow-up should increase and/or EUS with FNA should be considered.
(2) Cyst size directs follow-up or intervention. Although our cyst size thresholds (ie, <1.5 cm, 1.5-2.5 cm, >2.5 cm) differ from the commonly used 3 cm threshold, our choices are sensitive to studies of surgically resected “Sendai-negative” cysts <3 cm, which have shown that high-grade dysplasia or frank malignancy may occur in cysts of this size.
(3) Because the flowcharts apply to a range of cyst sizes, growth may require shifting from one flowchart to another, most commonly when a cyst grows from <1.5 to >1.5 cm. Such shifts may also be appropriate when a cyst is first discovered in patients who are close to 80 years of age, as described above). In general, a new 9- to 10-year follow-up period is not recommended when such a shift occurs; rather, decisions concerning total follow-up length should be tailored to the patient’s circumstance. Alternatively, it is appropriate to consider direct sampling of a growing cyst (ie, EUS and FNA).
(4) Development of “worrisome features” or “high-risk stigmata,” as described above (“Reporting Considerations” section), should prompt EUS/FNA and surgical consultation. The exception is that cysts ≥3 cm without any additional “worrisome features” or “high-risk stigmata” can alternatively be followed.
(5) Comparison with prior imaging studies is crucial, including those where the pancreas is frequently visualized, such as chest CT, spine CT or MRI, PET/ CT, and abdominal ultrasound. Prior studies should be reviewed for stability and features. The date of a prior study can be used as a baseline to establish a follow-up schedule.Regardless of the modality, intravenous contrast, multiphase acquisitions, and thin sections for 3D visu- alization are generally needed. Sixteen-slice or greater multiple detector CT scanners acquire submillimeter slices with isotropic voxels and allow reformatted thicker slices (3-5 mm). Pancreatic-phase images should begin about 50 seconds after initiating the intravenous contrast injection. Injection rates of 4-5 mL/s may optimally display peripancreatic vasculature and maximize pancreatic enhancement. A second phase is recommended at approximately 80 seconds to evaluate the liver. Management of Incidental Pancreatic Cysts: A White Paper of the ACR Incidental Findings Committee.
Megibow AJ et al. J Am Coll Radiol. 2017 Jul;14(7):911-923.







- OBJECTIVE. The purpose of this study is to retrospectively evaluate the differential CT features of isolated benign and malignant main pancreatic duct (MPD) dilatation and to investigate whether the diagnostic performance of radiologists can be improved with knowledge of these differential CT features.
CONCLUSION. Distal, long (≥ 6.1 mm), and abrupt transition, the absence of duct penetrating sign, and the presence of attenuation difference and PD or CBD enhancement were highly suggestive CT ndings for differentiation of malignant from benign MPD dilatation. The diagnostic performance of radiologists with regard to differentiation was signi cantly improved with knowledge of these highly suggestive CT criteria.
Isolated Main Pancreatic Duct Dilatation: CT Differentiation Between Benign and Malignant Causes Se Woo Kim et al AJR 2017; 209:1046–1055 - “In a 2013 study of the National Cancer Institute (NCI) Surveillance, Epidemiology, and End Results (SEER) registry, the estimated number of pancreatic cysts in the U.S. population between 40 and 84 years old was 3,428,874, with an overall cyst prevalence of 2.5%. Increased use of cross-sectional imaging has led to increased detection of such cysts in recent years; 2.2% of upper abdominal CT examinations and 19.6% of MRI examinations report a pancreatic cyst .”
Management of Incidental Pancreatic Cysts: A White Paper of the ACR Incidental Findings Committee. Megibow AJ et al. J Am Coll Radiol. 2017 Jul;14(7):911-923.
- “Facebook Live is a free, easy-to-use, and easy-to-access online resource for live, interactive educational delivery, which has quickly become one of our most popular social media channels. This venue provides students, trainees, and medical providers around the world with unprecedented access to leaders in the field. Educators interested in delivering free medical education resources on a global scale should engage in this activity.”
Facebook Live: A Free Real-Time Interactive Information Platform. Johnson PT, Thomas RB, Fishman EK. J Am Coll Radiol. 2017 Nov 1. pii: S1546-1440 - “Facebook Live” was created as a way for users to communicate to their friends and followers in real-time. Clicking the “go live” button within Facebook automatically engages your computer’s camera and microphone and begins streaming a live video. Along with the video, this platform also has a comments section, which allows the host and viewers to post and respond to comments during the live feed. Once the live feed has ended, Facebook automatically posts the recording to the user’s Facebook page for further viewing and commenting.”
Facebook Live: A Free Real-Time Interactive Information Platform. Johnson PT, Thomas RB, Fishman EK. J Am Coll Radiol. 2017 Nov 1. pii: S1546-1440 - “Based on user feedback, CTisus recognized one limitation to Facebook Live is the ability to show images (ie, digital CT scans), which is a major component in radiology education. With the recommendation of a viewer, CTisus began using a third-party screen-sharing software, OBS (Panama City, Panama). This free tool allows you to stream a split screen between live video and PowerPoint (Microsoft, Redmond, Washington, USA) without compromising sound or image quality. The downside to using this third-party software is that real-time comments are not present in the OBS window. However, this can be resolved by setting up another device to open Facebook and view the comments alongside OBS. OBS takes a few more steps to set up the live stream than using Facebook independently, but it greatly improves the educational opportunity for the viewers.”
Facebook Live: A Free Real-Time Interactive Information Platform. Johnson PT, Thomas RB, Fishman EK. J Am Coll Radiol. 2017 Nov 1. pii: S1546-1440
- Post-stent CT findings
Normal
• Aneurysm sac decreases in size progressively
Complications
• Aneurysm size increasing (endoleak)
• Change in stent positioning (migration, kinking)
• Branch vessel compromise
• Infection
• Limb thrombosis
• Aneurysm formation elsewhere in aorta - Type I Endoleak
• Proximal or distal stent not in complete contact with aortic wall
• Diameter of aorta too large at stent landing zone
• Gap between stent and aortic wall allows blood to flow into aneurysm sac - “Type II endoleak is the most common endoleak. It is seen in 10% to 20% of patients at the completion of EVARs. The usual culprit is retrograde filling of an aneurysm sac by either a patent IMA or a lumbar artery. Fortunately, spontaneous resolution is noted in up to 50% to 60% of patients by 30 days.
” Overview of aortic aneurysm management in the endovascular era. Calero A, Illig KA. Semin Vasc Surg. 2016 Mar;29(1-2):3-17 - Type III Endoleak: Facts
A Type III endoleak arises from poor seal between components or frank component separation.
It is associated with aneurysm sac pressurization and increased risk of rupture. It must be treated when found.
It can be treated with either a relining stent for poor seal or aorto-uni-iliac devices and femoral−femoral bypass for component separation - Type IV Endoleak: Facts
Type IV endoleak refers to the diffuse contrast blush occasionally seen immediately after implantation. This is a reflection of porosity of graft material and is usually self-limited and does not require treatment. - “Renal ischemia remains a known compli- cation of FEVAR, with clinical studies showing variable rates of renal impairment after FEVAR of juxtarenal abdominal aortic aneurysms. Studies show that 11– 35% of patients experience a transient increase in serum creatinine levels (defined as a > 30% increase in serum creatinine level), and 0–4% of patients require temporary or permanent dialysis.” Incidence and Clinical Significance of Renal Infarct After Fenestrated Endovascular Aortic Aneurysm Repair Burke LMB et al. AJR 2017; 208:885–890
- “Our data show a gradual mild increase in baseline serum creatinine level in all patients undergoing FEVAR, regardless of whether the patient had a renal infarct. This finding mirrors a recent study from France , which found an increase in serum creatinine level during the first week after FEVAR.”
Incidence and Clinical Significance of Renal Infarct After Fenestrated Endovascular Aortic Aneurysm Repair Burke LMB et al. AJR 2017; 208:885–890
- Abdominal Aortic Aneurysm
Aneurysm defined as:
• Diameter >3.0 cm
• Dilated region with diameter >50% of normal region (1.5x its normal size)
Causes:
• Hypertension/smoking
• Connective tissue disorders/familial
• Infection (mycotic aneurysm) - Abdominal Aortic Aneurysm: Facts
• The infrarenal aorta is the most common site of aortic aneurysm formation
• Aortic aneurysms are three to four times more common in men than in women
• The incidence in men older than 60 years of age is 4% to 8%, while that in women is 0.5% to 2%
• Risk factors for AAA include age, hypertension, chronic obstructive pulmonary disease (COPD), history of cigarette smoking, male sex, and family history of an aortic aneurysm.
• The prevalence of AAA among those who had a first-degree relative with an AAA is as high as 30% - Abdominal Aortic Aneurysms: Genetic Disease
• Type IV Ehlers-Danlos syndrome
• Marfan syndrome
• Loeys Dietz syndrome - Thresholds for AAA repair
Abdominal Aorta:
• Fusiform > 5.5 cm warrants repair (1-year incidence of rupture was 9.4% for AAAs measuring 5.5 to 5.9 cm, 10.2% for AAAs of 6.0 to 6.9 cm, and 32.5% for AAAs of ≥7.0 cm)
• Rapid growth > 1cm/yr
• Symptomatic AAA should be repaired
• Consider elective repair of any saccular aneurysms - “Endovascular aneurysm repair (EVAR) has become the standard of care (given appropriate anatomy) based on its lower morbidity and mortality compared with open surgery. The use of EVAR continues to be limited by anatomic factors, including neck angulation, a short or wide neck, severe calcification, access difficulties, and the presence of thrombus, but modern grafts implanted in patients with proper anatomy seem to be extremely durable.” Overview of aortic aneurysm management in the endovascular era. Calero A, Illig KA. Semin Vasc Surg. 2016 Mar;29(1-2):3-17