Cinematic Rendering: Principles, Applications, and Observations in CTMandibular Fracture 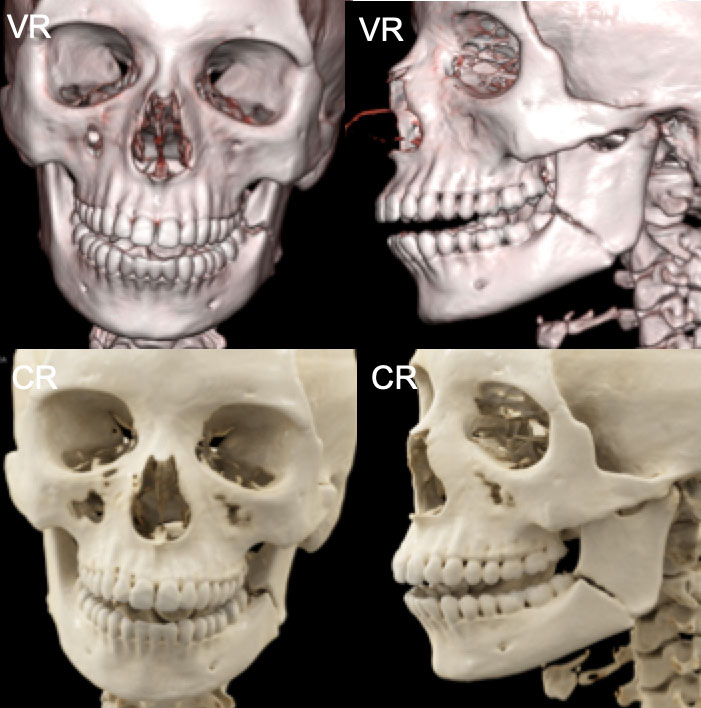 |
Multiple Facial Fractures 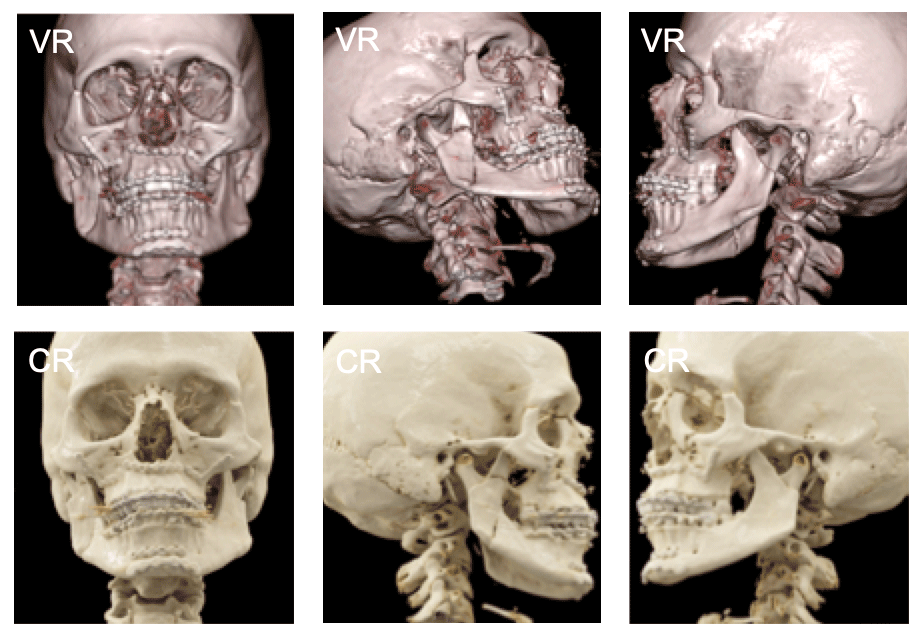 VR vs. CR: multiple facial and mandibular fractures |
Polyostotic Fibrous Dysplasia 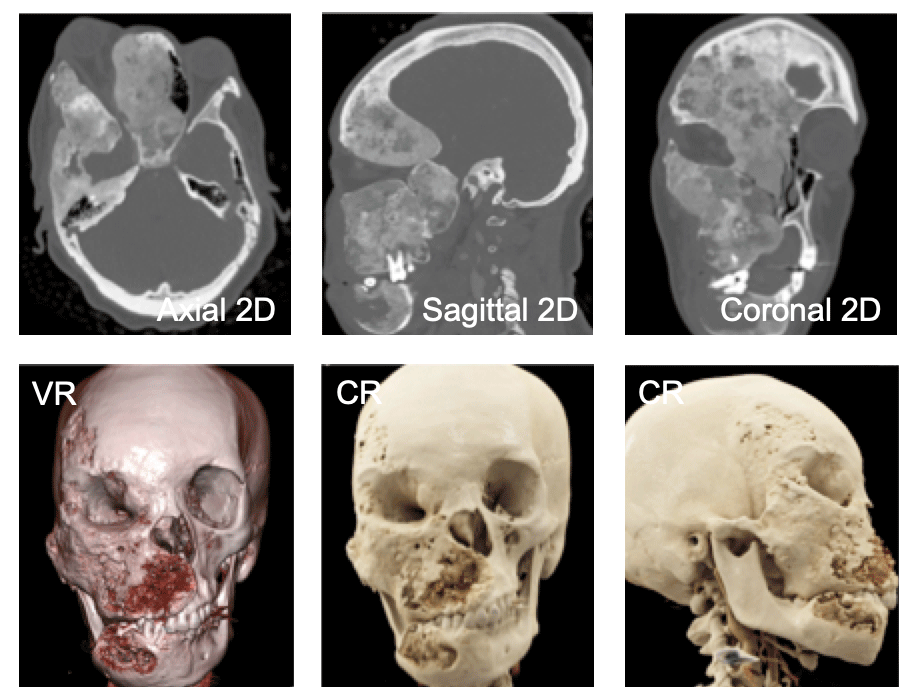 The profound deformation of the right orbit is best appreciated on the cinematic renderings in the lower right due to the realistic shadowing effects created by this method |
Gunshot Wound with Extensive Facial Fractures 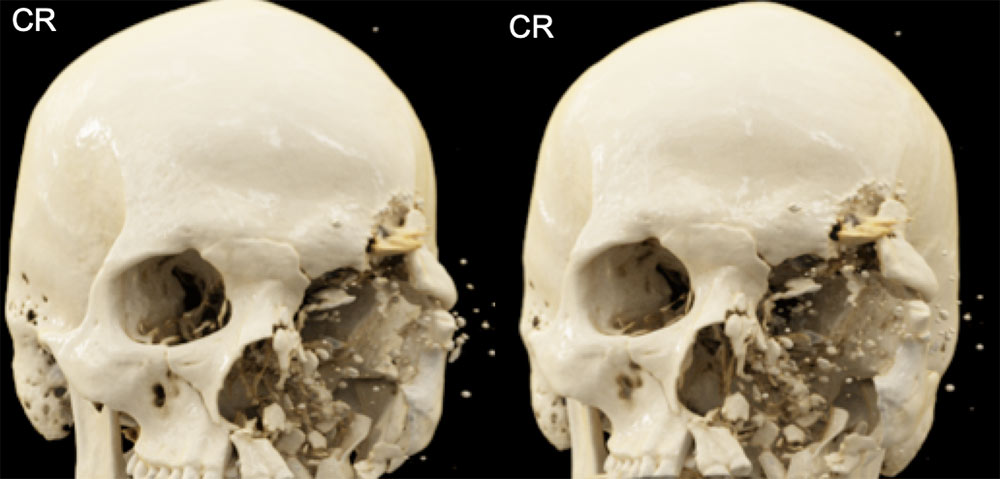 The extensive comminution of the fractures and their relative positions are easily appreciated with CR |
Cinematic Vs. Volume Rendering for Soft Tissue Evaluation  The ultra-high surface detail that is possible with cinematic rendering can highlight tendons extremely reliably – thus cinematic rendering may play an adjunct role to, or even replace, MRI in certain situations such as the emergency room setting. Rowe SP, Fritz J, Fishman EK. Emerg Radiol. 2017; Ahead of print. |
Tibial Plateau and Fibular Fractures 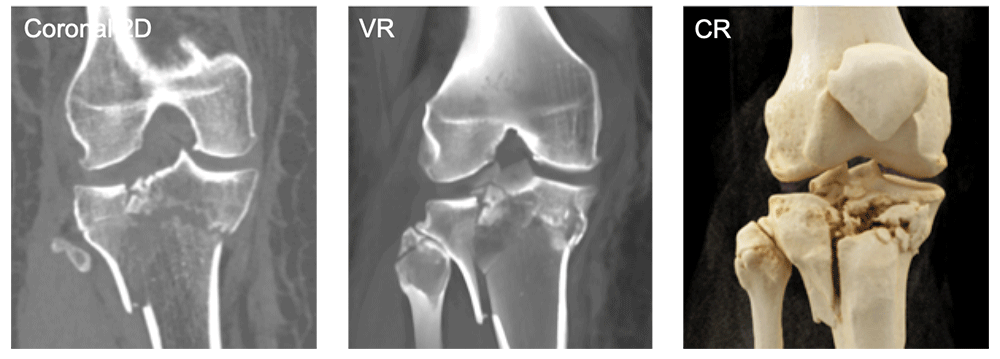 Photorealistic depictions of complex fractures may aid surgeons in pre-operative planning Rowe SP, Fritz J, Fishman EK. Emerg Radiol. 2017; Ahead of print. |
Soft Tissue Injuries are Well-Delineated by Cinematic Rendering 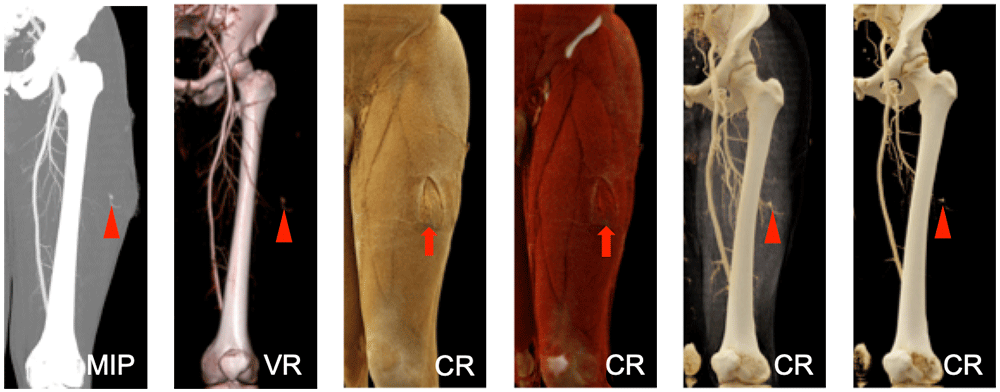 Soft tissue injuries (red arrows), vascular injuries (red arrowheads), and bone structures are all well-shown by CR Rowe SP, Fritz J, Fishman EK. Emerg Radiol. 2017; Ahead of print. |
Right Hip Fracture-Dislocation 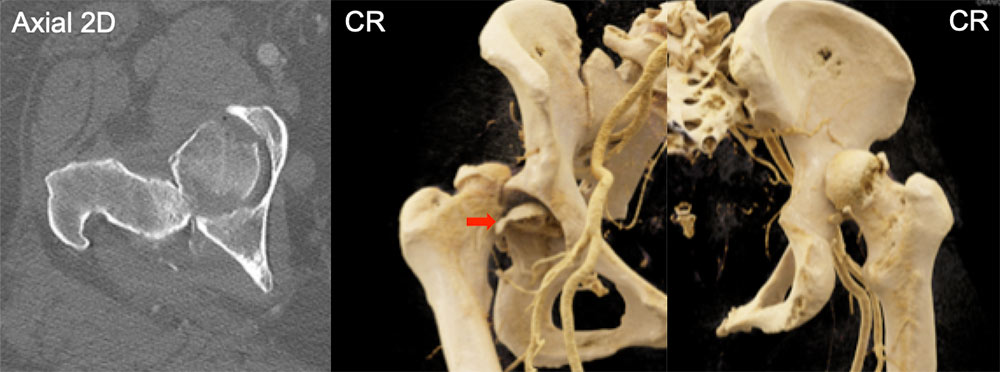 The displaced position of the posterior aspect of the right femoral head is well appreciated on the CR images; note also the realistic shadowing associated with the fractured portion of the femoral head that remains in the acetabulum (red arrow) |
Femoral Neck Fracture 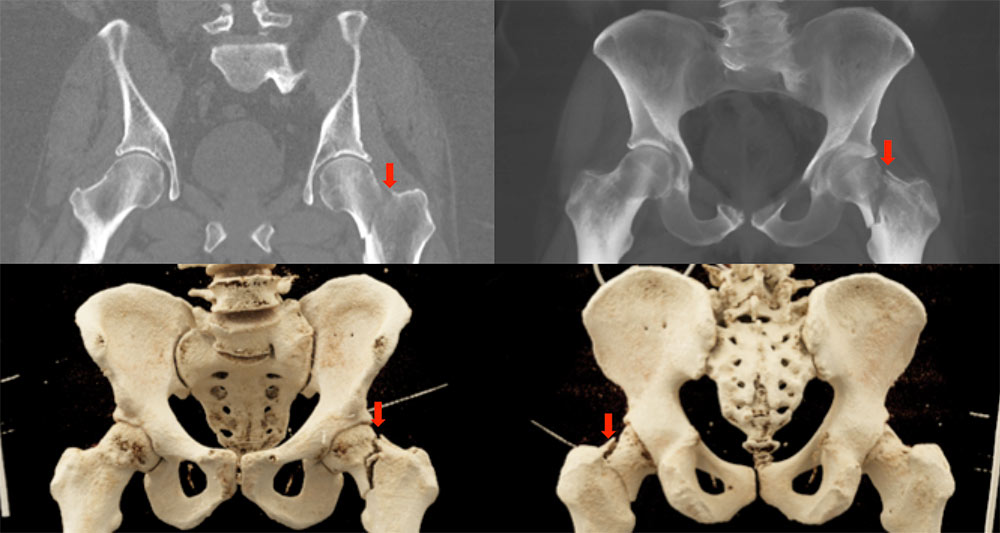 |
Hip Dysplasia 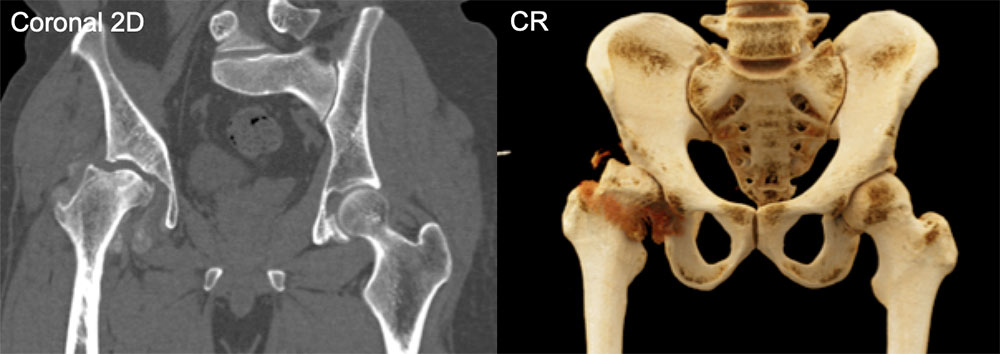 |
Ballistic Fracture of the Humerus 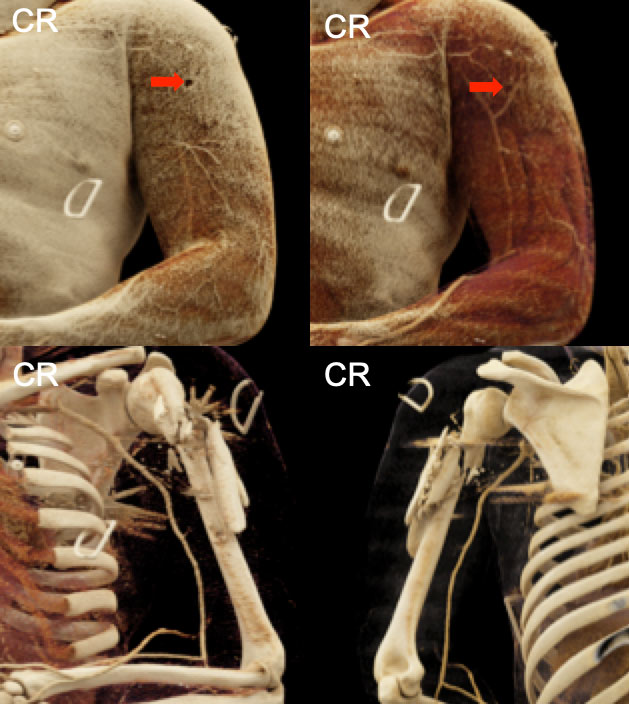 The subtle bullet hole in the soft tissues that caused this non-subtle extensively comminuted left humerus fracture can be appreciated in the top panels (red arrows) |
Radial Head Fracture and Elbow Joint Dislocation 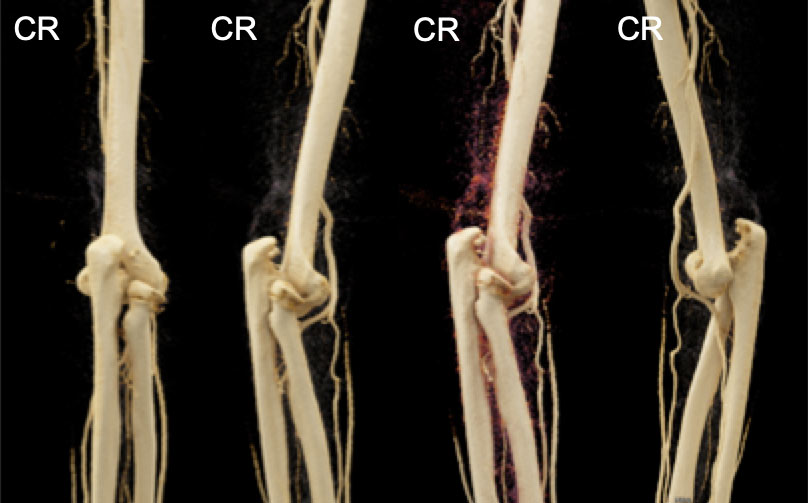 |
Stab Injury 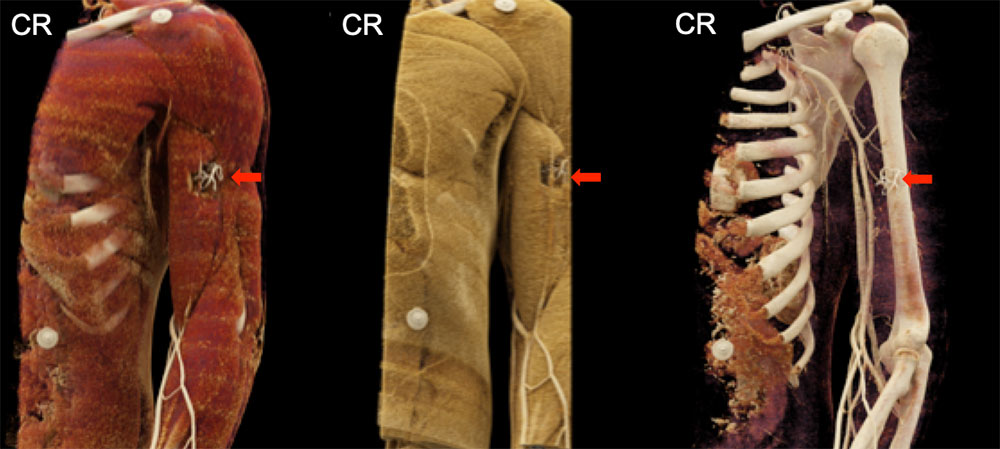 No major vascular or bone injury is appreciated; however the soft tissue injury to the biceps musculature with packing material is clearly delineated (red arrows) |
Distal Radius Fracture  |
Ankle Joint Dislocation with Fibula Fracture 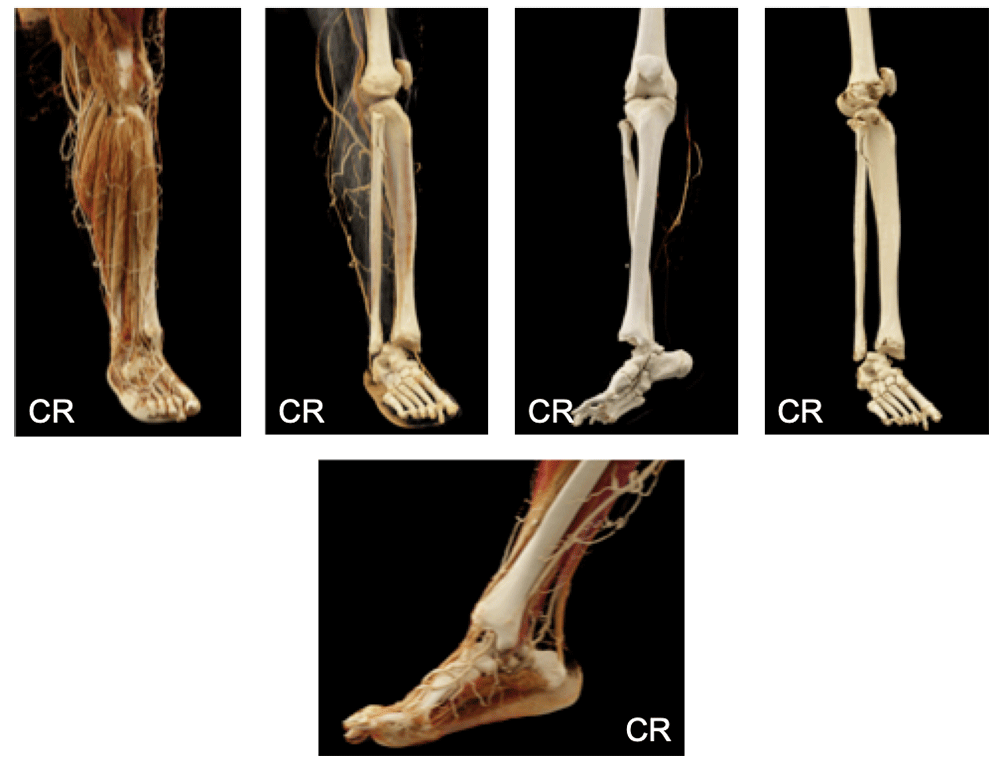 |
Dermatomyositis with Soft Tissue Calcifications 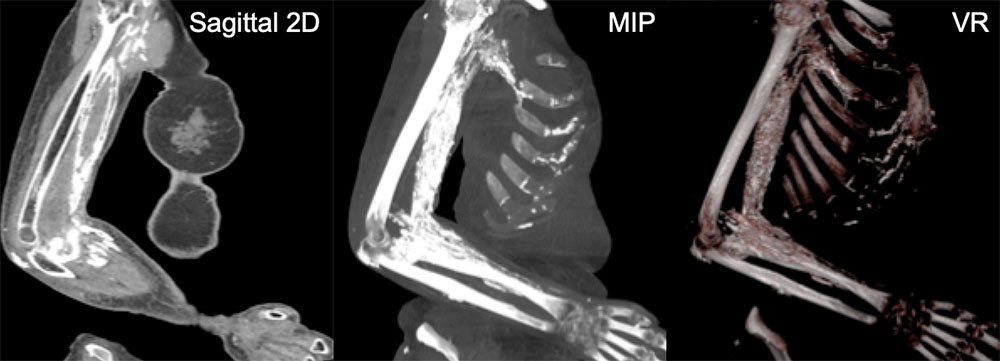 |
Dermatomyositis with Soft Tissue Calcifications 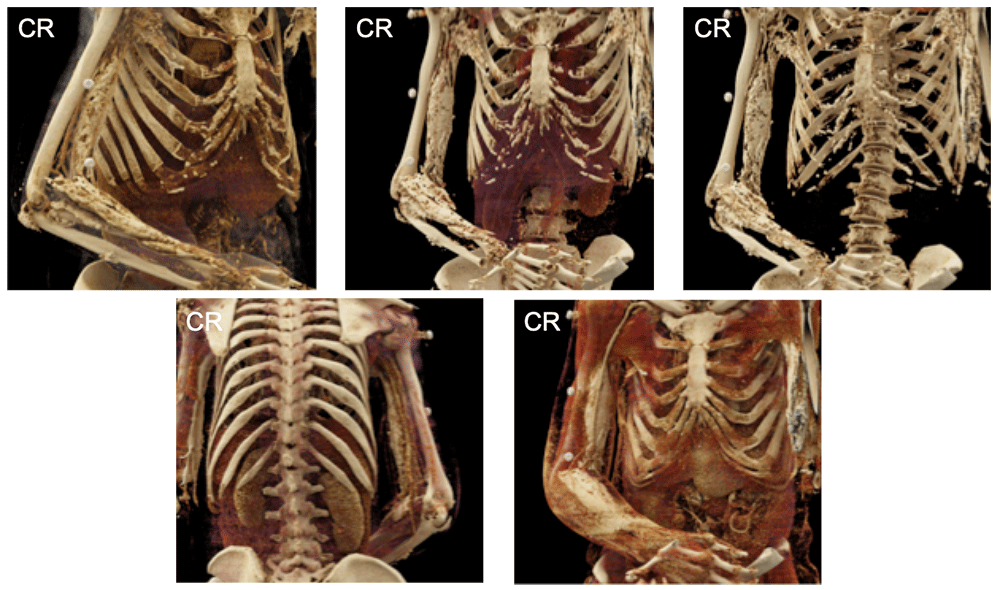 |
Coronary Artery to Pulmonary Artery Fistula 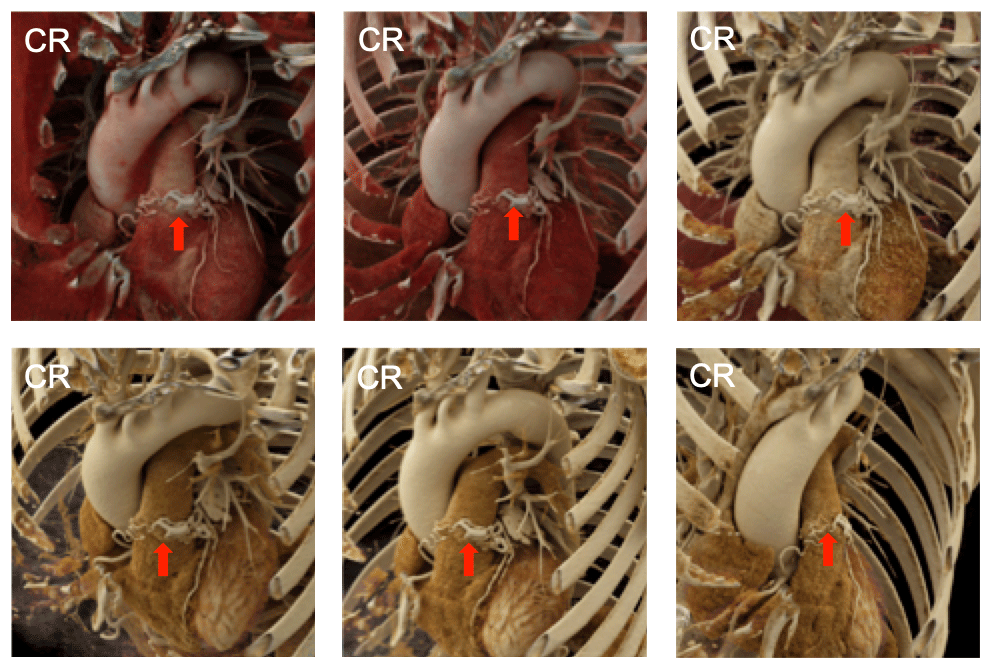 |
Ductus Diverticulum – Potential Pitfall for an Acute Aortic Injury 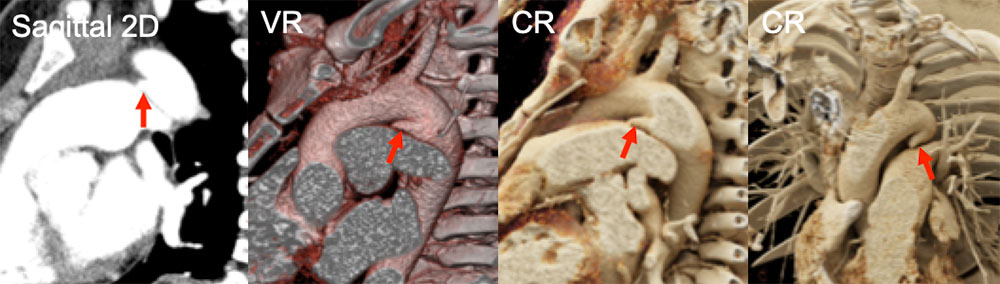 |
Ductus Diverticulum – Potential Pitfall for an Acute Aortic Injury 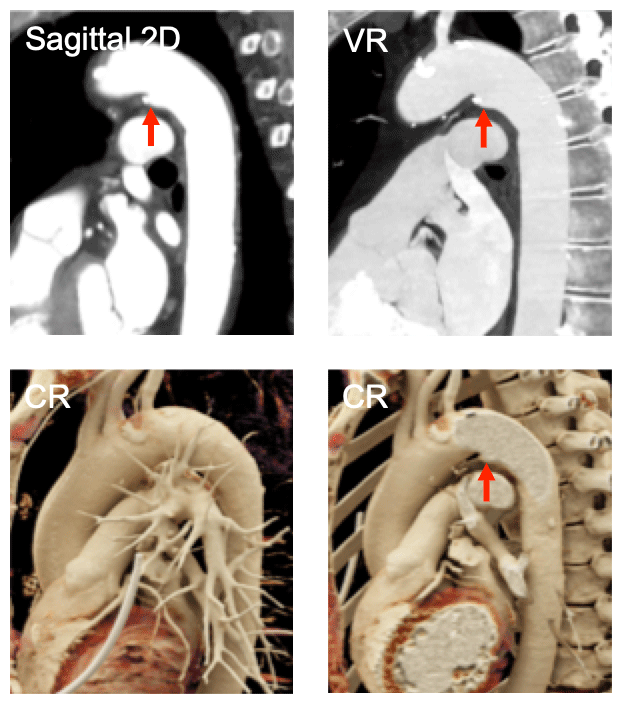 Note how in the image in the lower left that overlying vessels and other structures can obscure the light source and prevent visualization of the pathology |
Ductus Diverticulum – Potential Pitfall for an Acute Aortic Injury 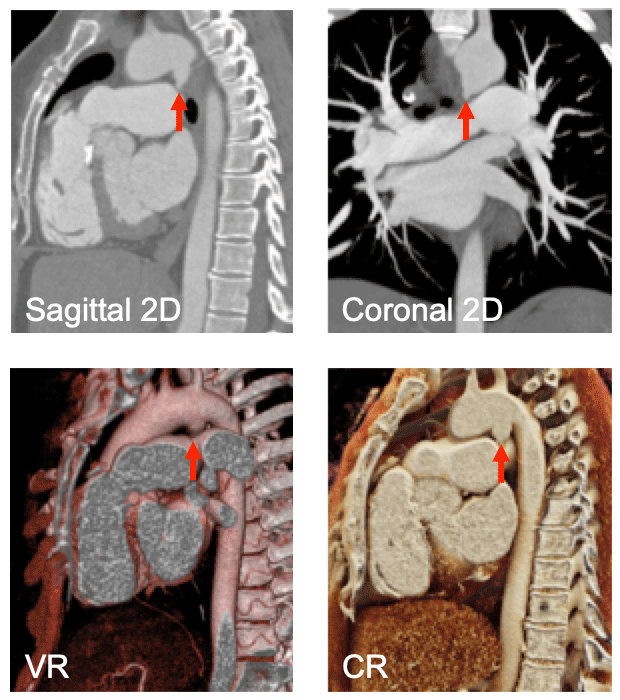 Ductus diverticula can acquire a number of different shapes, complicating the interpretation of these stuctures |
Acute Aortic Injury 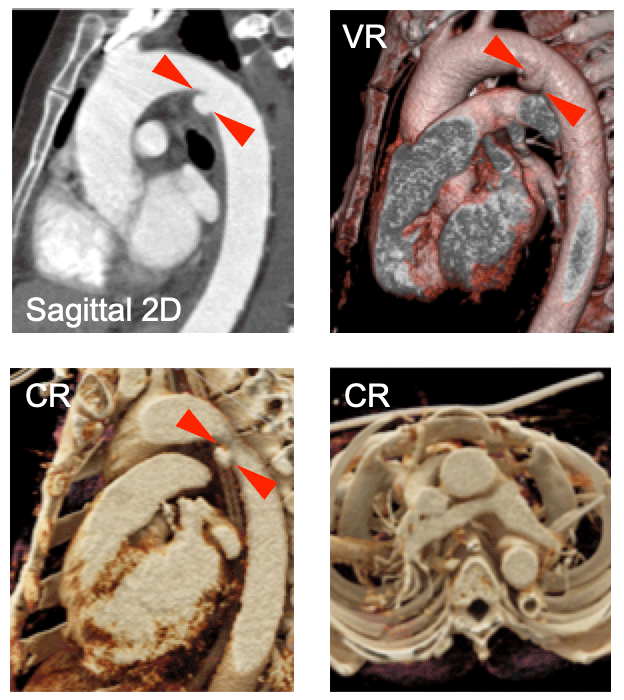 Note the acute angles (red arrowheads) between the aorta and this lesion, indicating it is a true acute aortic injury and not a ductus diverticulum |
Normal Anatomy: Highly Detailed View of the Left Atrial Appendage  |
Approximately 50% Stenosis in the LAD 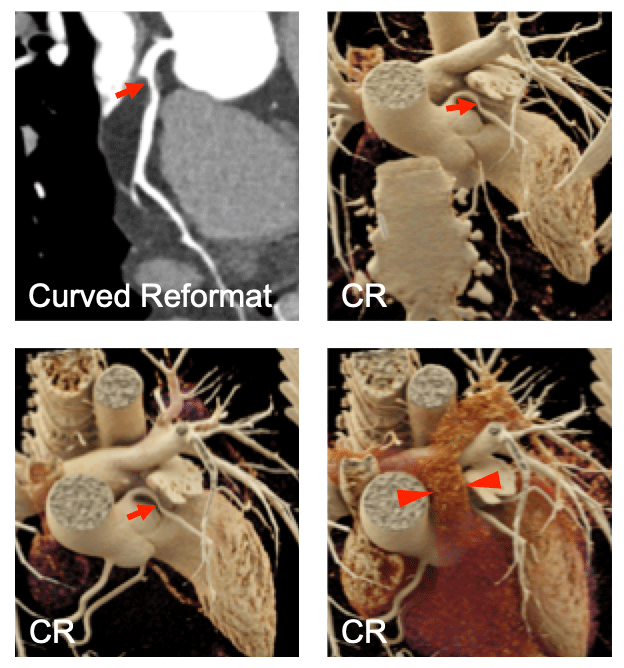 An LAD stenosis is identified (red arrows), but can be obscured with cinematic rendering (red arrowheads) if the operator does not carefully examine the volumetric data from a variety of different views and with varying widow widths/levels and transparency settings |
Intracardiac Spindle Cell Tumor 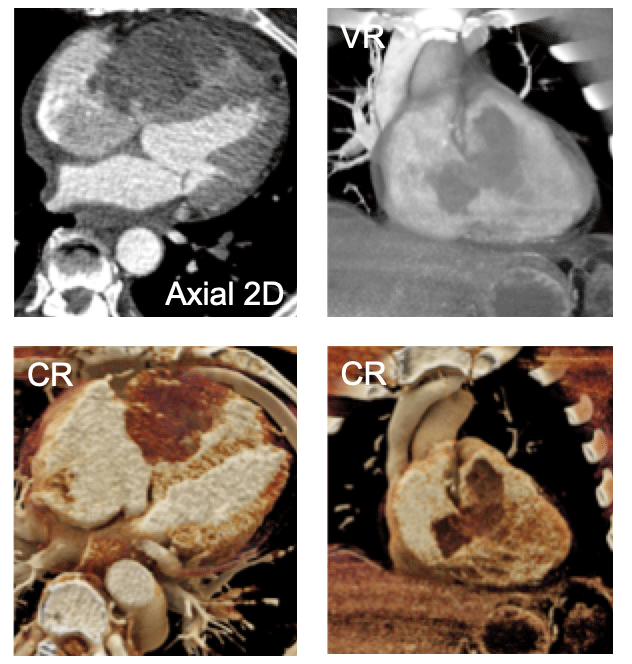 |
Abdominal Aortic Aneurysm 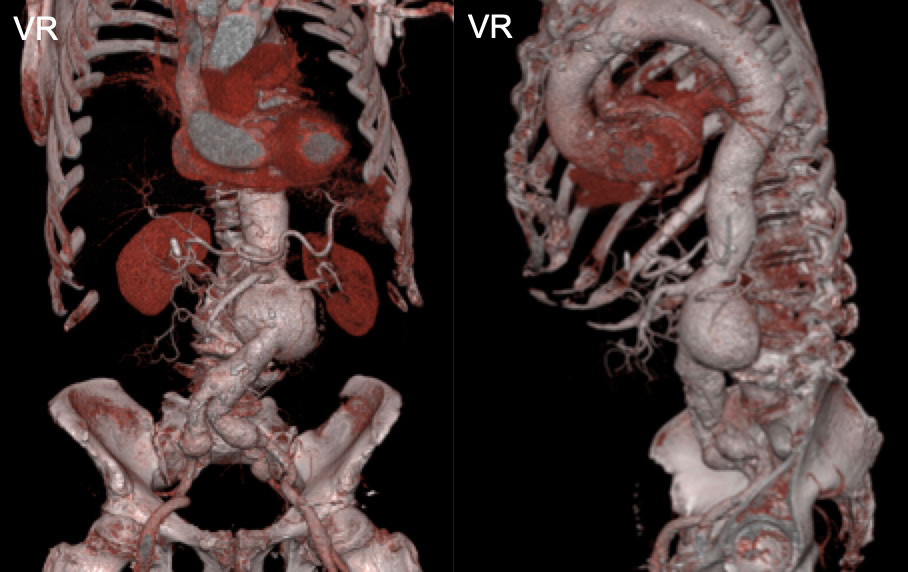 |
Abdominal Aortic Aneurysm 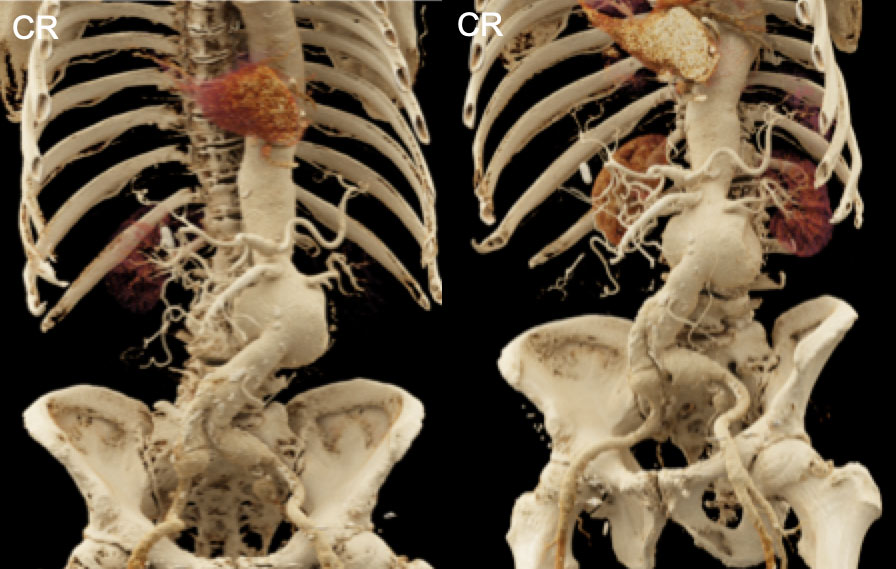 Relative to the VR images on the previous slide, these CR images provide more realistic shadowing effects that create depth in the image that may be helpful when surgeons are planning a necessary intervention |
Peripheral Vascular Grafts in a Patient with Loeys-Dietz Syndrome 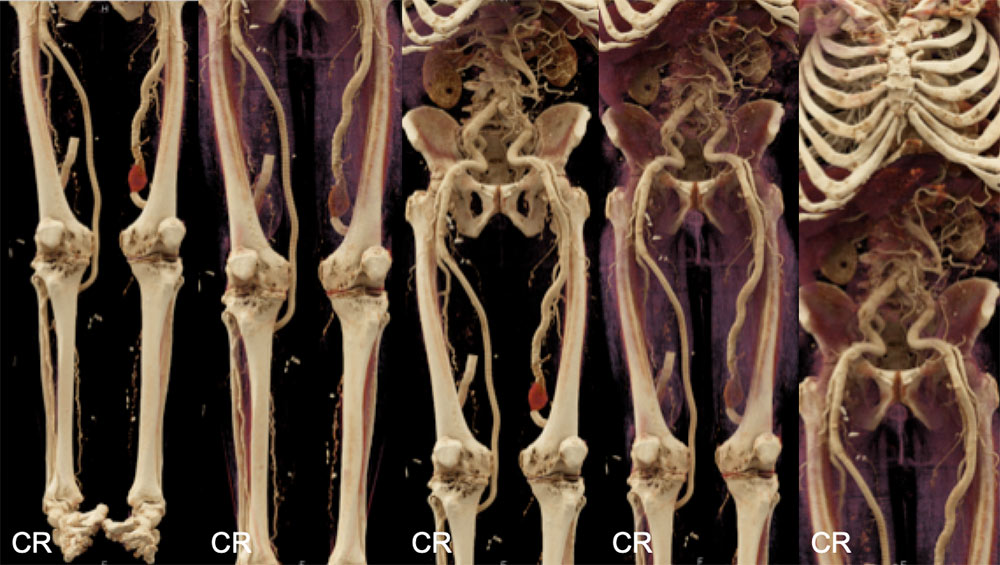 |
Renal Artery Fibromuscular Dysplasia 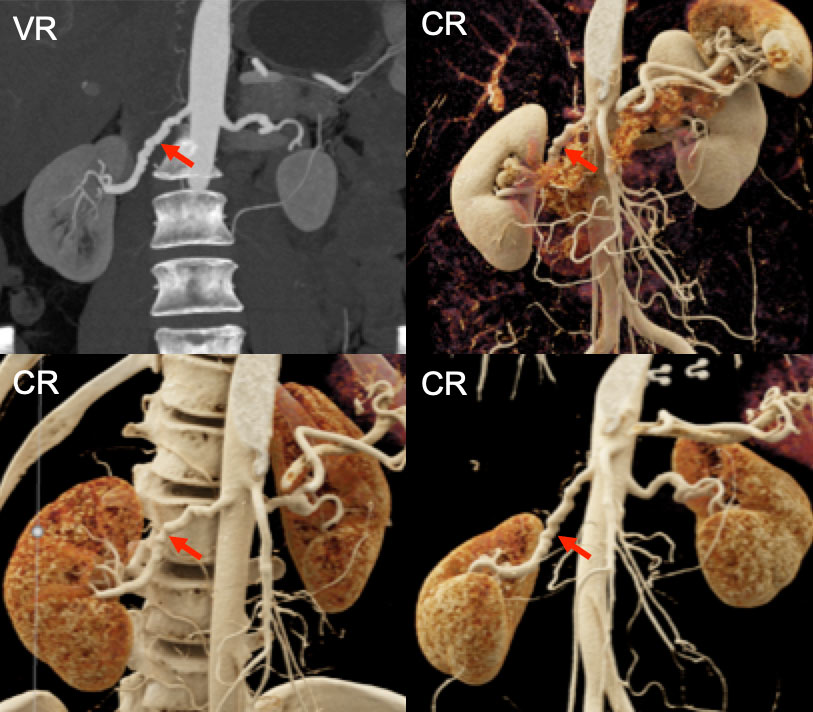 The ability of including or excluding soft tissue during CR can allow for very high contrast such as can be seen in the right renal artery with fibromuscular dysplasia (red arrows), particularly in the bottom right panel |
Distal Aortic Occlusion with Collateral Vessel Formation 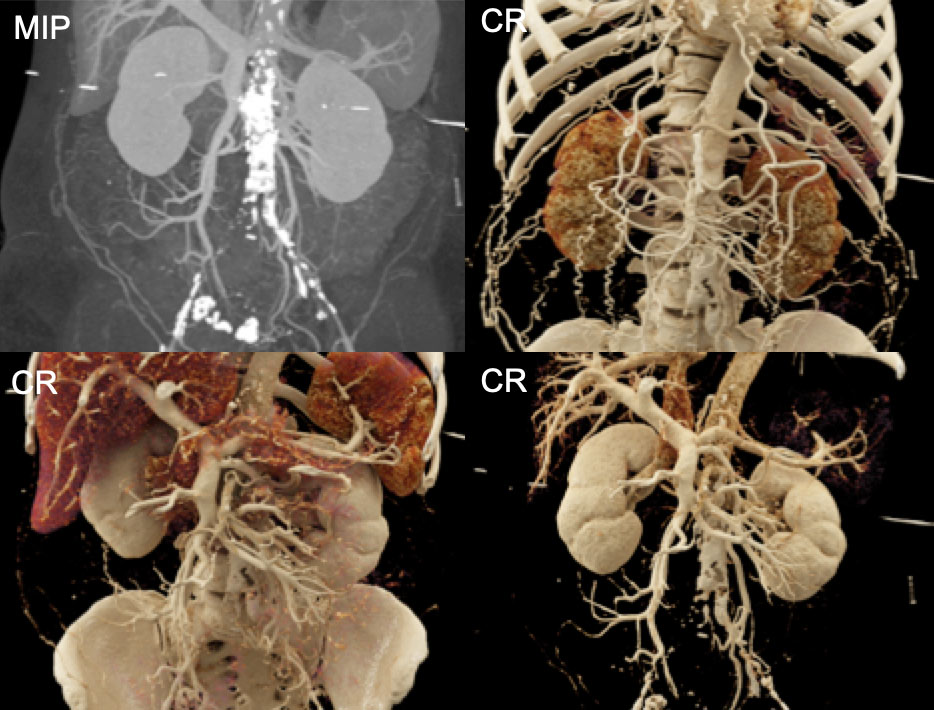 |
Distal Aortic Occlusion with Collateral Vessel Formation 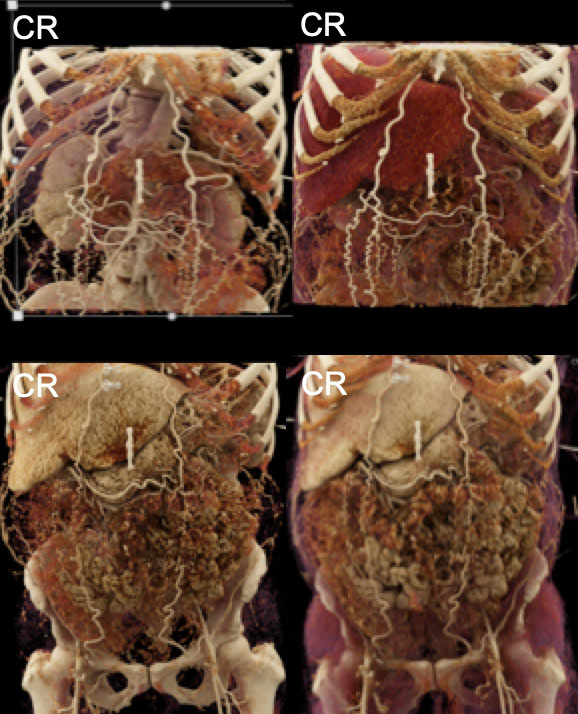 |
Right Kidney Xanthogranulomatous Pyelonephritis 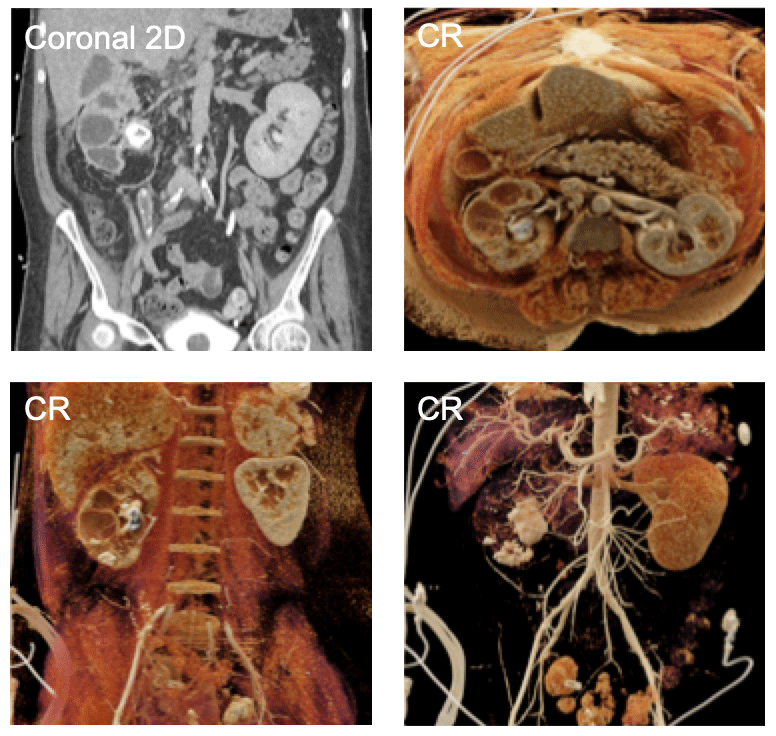 Note the staghorn calculus in the renal pelvis with multiple additional stones layering in the dilated/cystic calyces |
Bilateral Staghorn Calculi 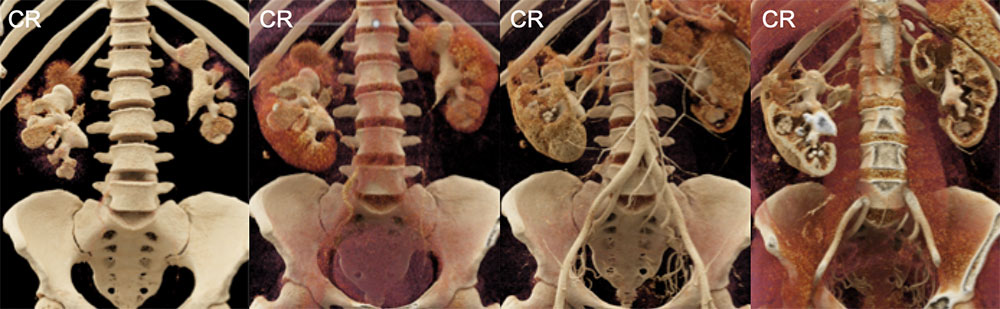 |
Bilateral Asymptomatic Ureteropelvic Junction Obstructions 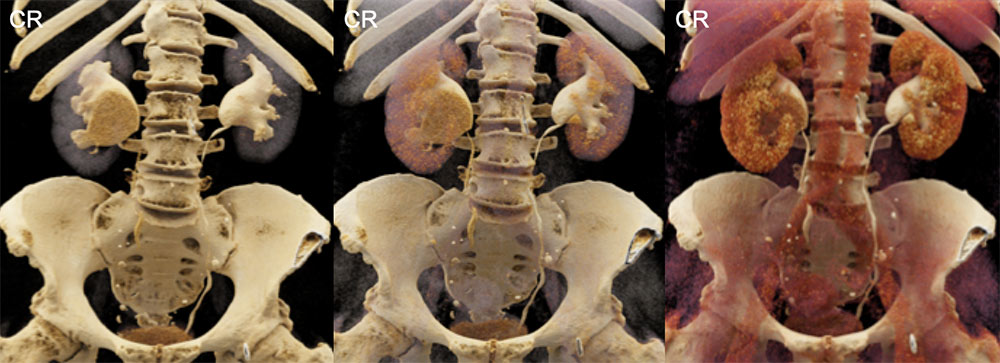 |
Ureteropelvic Junction Obstruction Due to Crossing Vessel  |
Ureticopelvic Junction Obstruction Due to Crossing Vessel 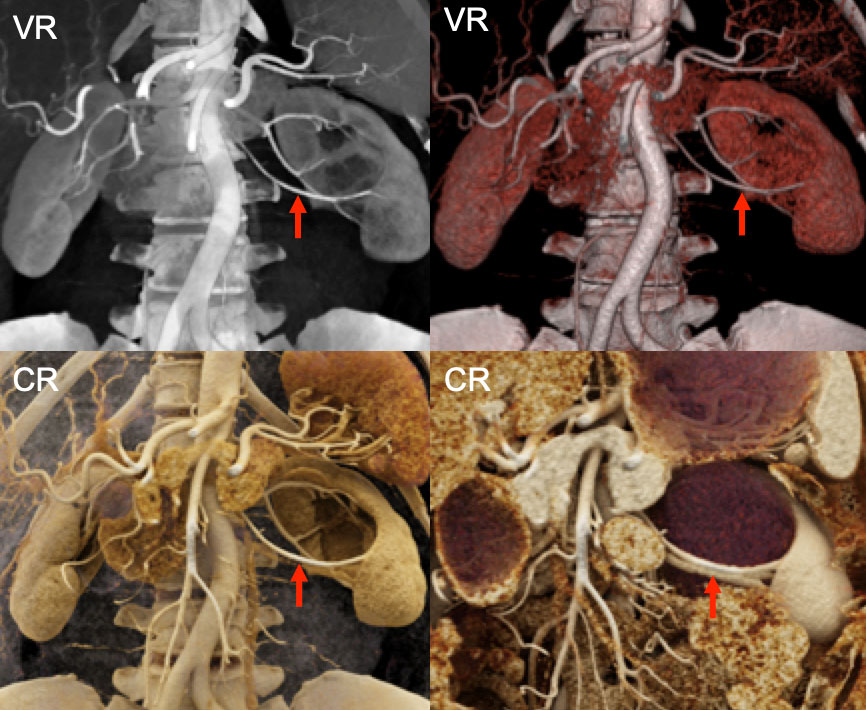 The crossing vessel (red arrow) that has lead to the UPJ obstruction is visible with both VR and CR |
Cross-Fused Renal Ectopia 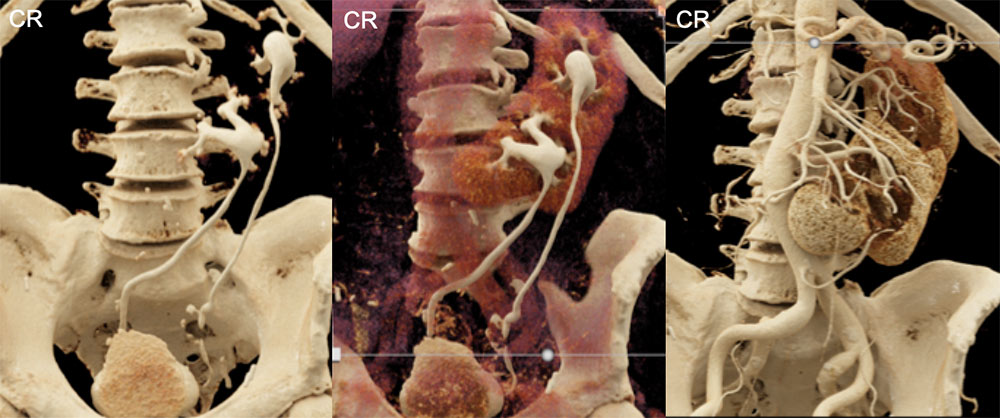 |
Crohn’s Disease with the Comb Sign 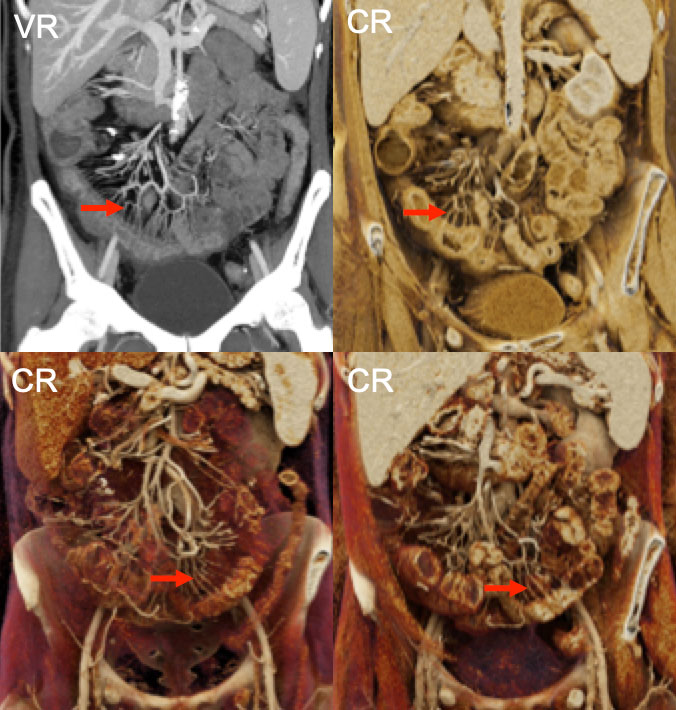 Long-standing inflammatory bowel disease can manifest increased mesenteric vasculature (the comb sign, red arrows), which is well appreciated on 3D images such as on CR |
Upper Gastrointestinal Hemorrhage 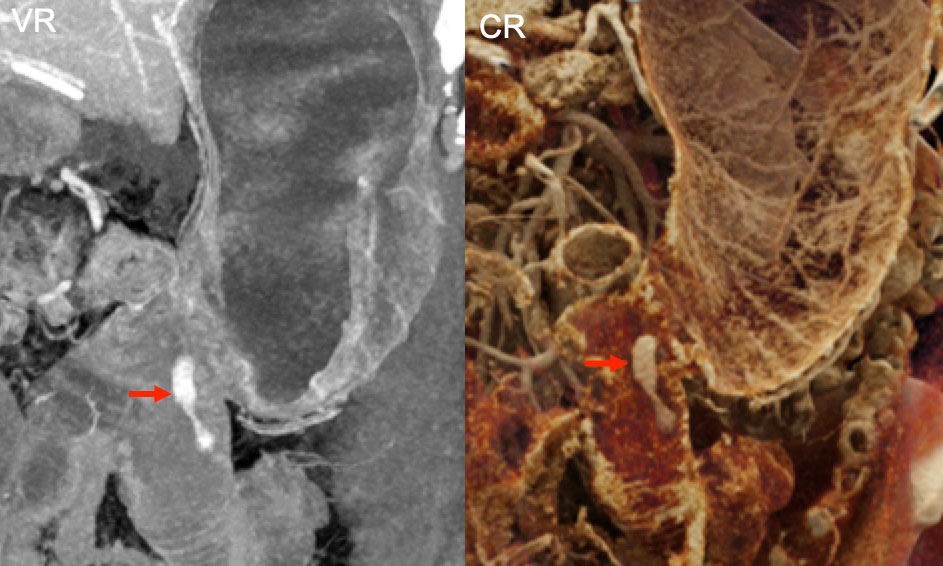 Active hemorrhage (red arrows) at site of prior gastro-jejunostomy |
Volvulus with Small Bowel Obstruction 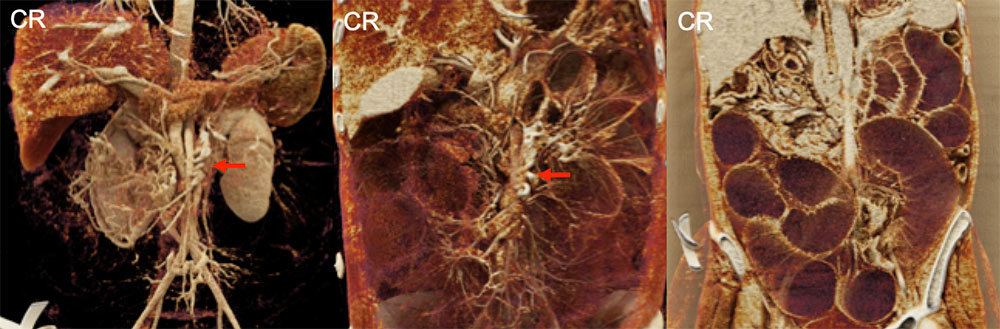 Note both the swirled appearance of the mesenteric vasculature (red arrows) as well as the massively dilated loops of obstructed small bowel |
Cirrhosis with Recanalized Umbilical Vein and Ascites 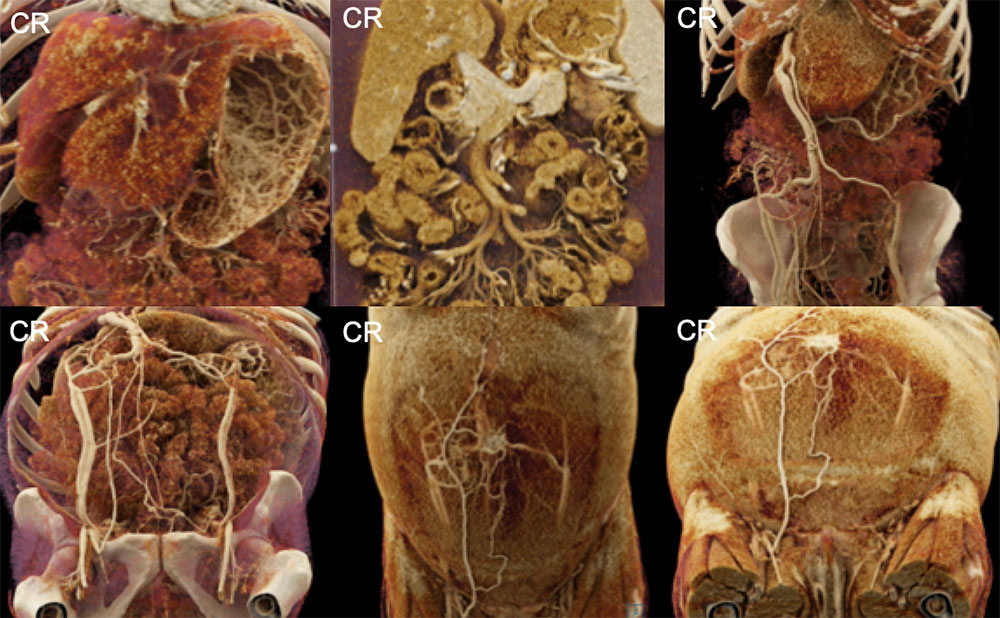 |
Future Directions
|
Future Directions
|
References and Further Reading Dappa E, Higashigaito K, Fornaro J, et al. Insights Imaging. 2016;7:849-856. Eid M, De Cecco CN, Nance JW Jr, et al. AJR Am J Roentgenol. 2017;209:370-379. Johnson PT, Schneider R, Lugo-Fagundo C, et al. AJR Am J Roentgenol. 2017;209:309-312. Rowe SP, Fritz J, Fishman EK. Emerg Radiol. 2017; Ahead of print. Rowe SP, Fishman EK. Radiol Case Rep. 2017; Ahead of print. Rowe SP, Johnson PT, Fishman EK. Br J Radiol. 2017; Ahead of print. |
