Acute Vascular Pathology: Distinguishing Abdominal Pseudoaneurysms from Aneurysms and Implications for Patient ManagementAcute Vascular Pathology: Distinguishing Abdominal Pseudoaneurysms from Aneurysms and Implications for Patient Management F Verde, MD |
Objectives
|
MDCT Protocol Design
|
Limitation of Oral Contrast Where is the pseudoaneurysm?? 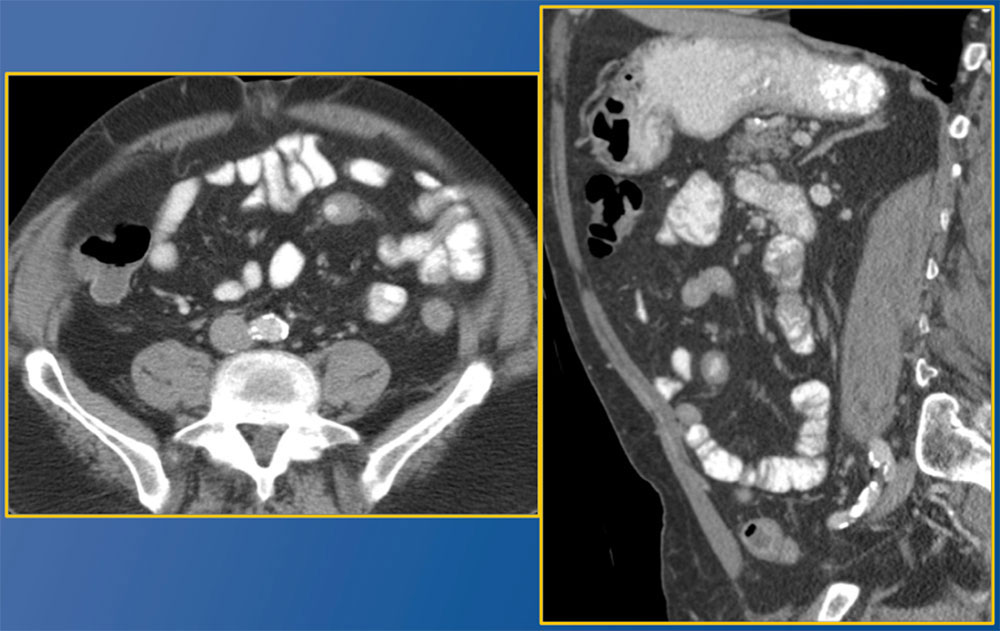 |
Limitation of Oral Contrast Post traumatic mesenteric artery pseudoaneurysm (red arrow). More conspicuous on follow up study with oral contrast only in colon (B) and on coronal MPR (C), which shows mesenteric stranding (yellow arrow). 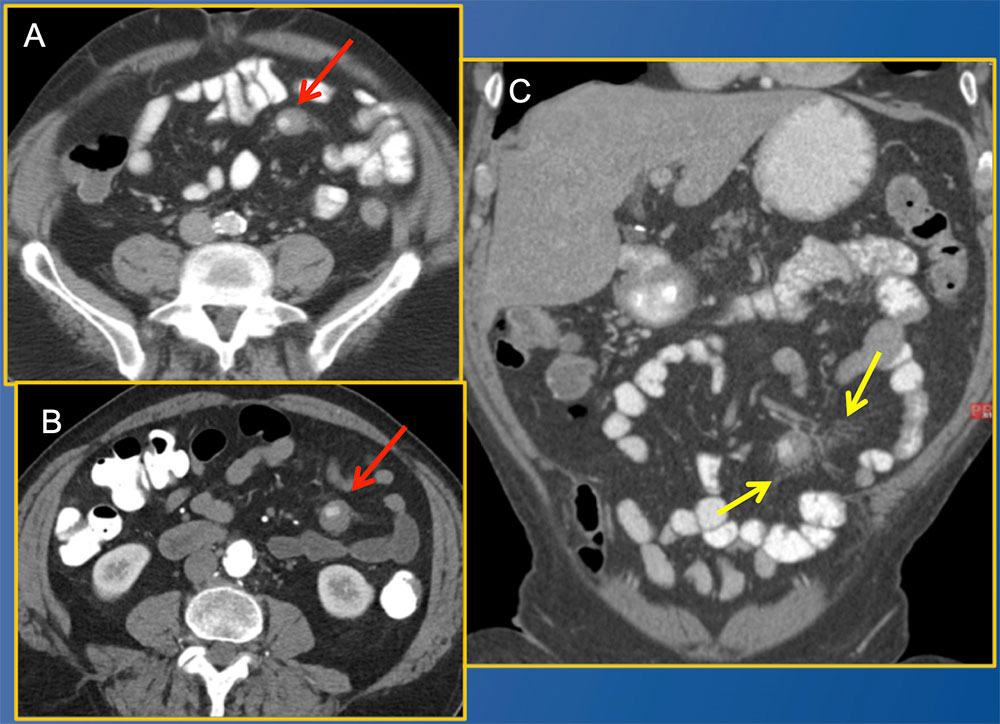 |
Dual Phase MDCT Pearls Some pseudoaneurysms and large aneurysms require time to fully opacify
|
GDA Pseudoaneurysm: Delayed Enhancement GDA pseudoaneurysms are fed by small branches and may enhance more on venous phase. 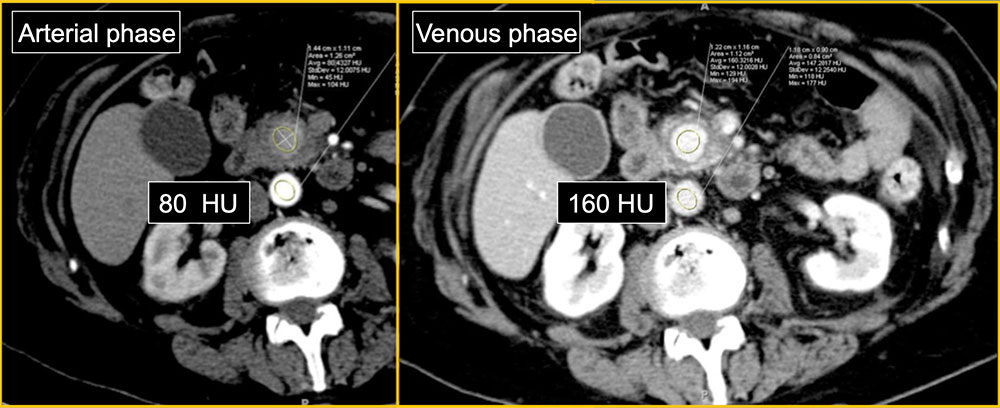 |
GDA Pseudoaneurysm: Delayed Enhancement GDA pseudoaneurysms are fed by small branches and may enhance more on venous phase. 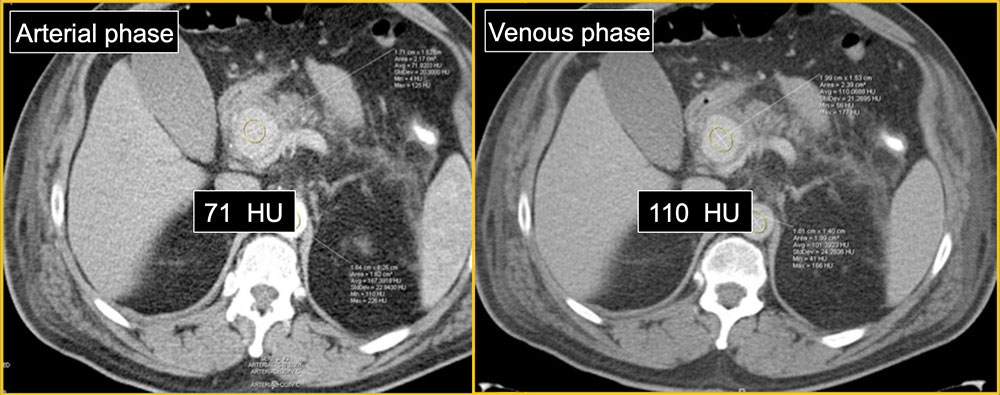 |
Volumetric Post Processing
|
MPRs for Mesenteric Vasculature
|
Imaging Technique Role of multi-planar reconstructions
 |
Imaging Technique Role of multi-planar reconstructions
 |
Pathophysiology True aneurysm vs Pseudoaneurysm
|
True Aneurysm vs Pseudoaneurysm – Presentation 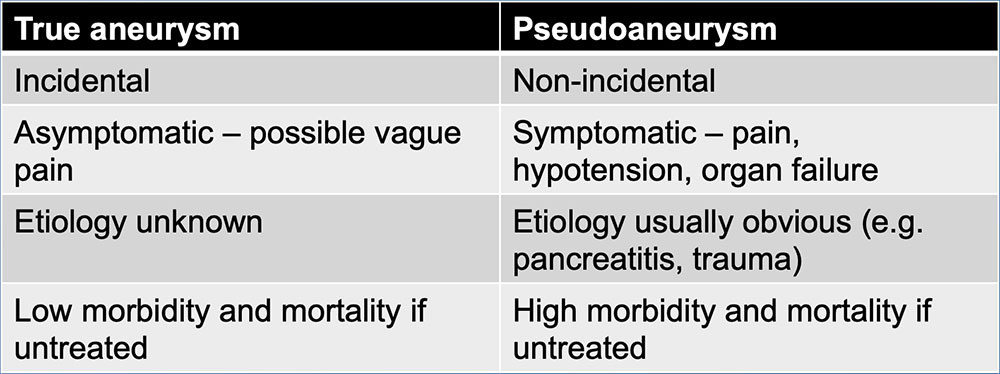 |
True Aneurysm vs Pseudoaneurysm - Common Etiologies 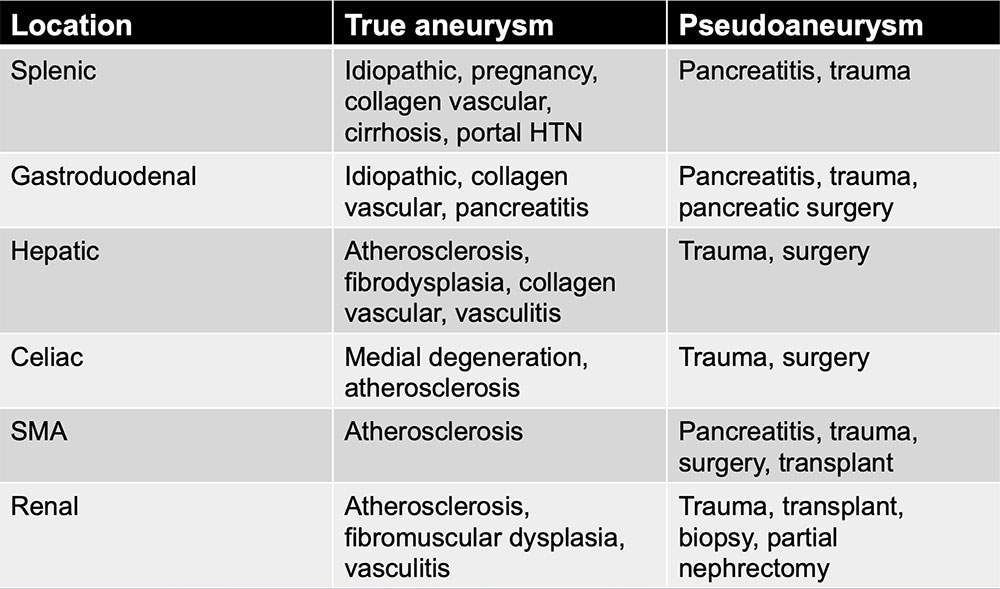 |
True Aneurysm vs Pseudoaneurysm - Imaging Summary 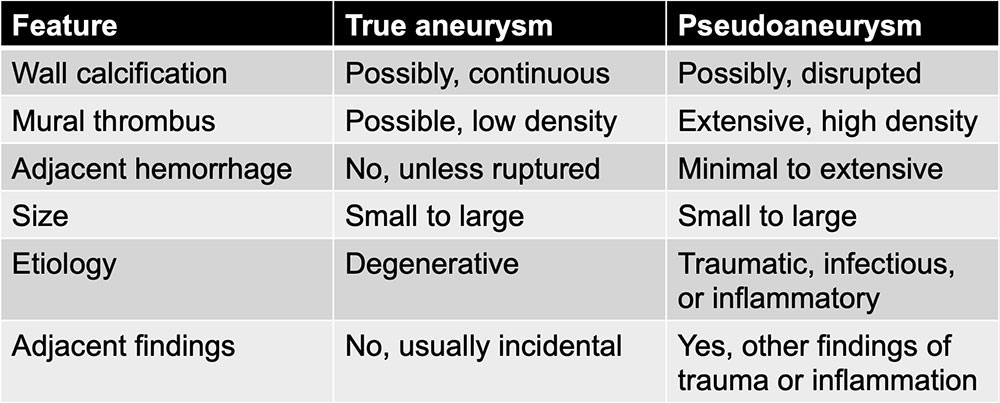 |
Mesenteric True Aneurysm Vessel Distribution
|
True Aneurysms: Splenic Artery Aneurysm 54-year-old woman with history of autoimmune hepatitis. Axial contrast-enhanced MDCT image shows 1.8-cm aneurysm (arrow) arising from splenic artery. Note lack of surrounding hemorrhage and other traumatic or inflammatory changes, consistent with a true aneurysm. 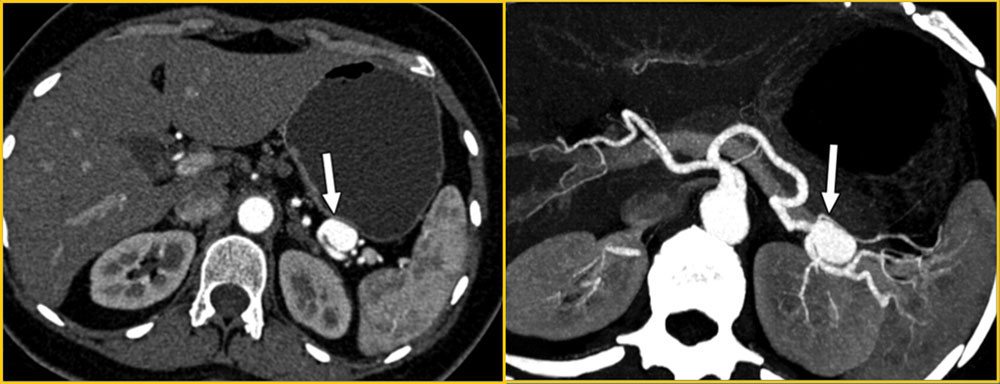 |
Splenic Artery Aneurysm Management
|
True Aneurysms: Hepatic Artery Aneurysm 60-year-old man with long history of hepatitis Axial CT (A) image shows 1.6-cm aneurysm (arrow) of common hepatic artery. Aneurysm is completely depicted with axial 3D rendering (B). Note lack of supporting findings so one may confidently diagnose a true aneurysm. 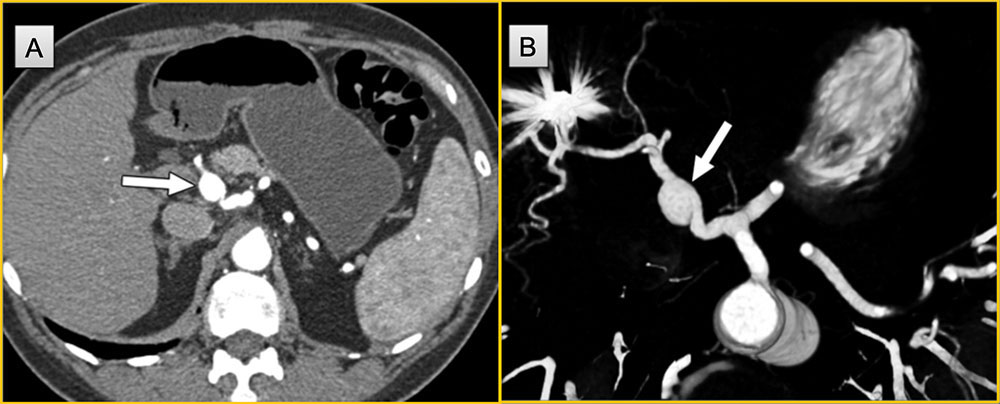 |
True Aneurysms: SMA Aneurysm 65-year-old man presenting with abdominal pain. Coronal thick slab MIP imaging demonstrating incidental small distal branch SMA aneurysm. Aneurysm is completely depicted in relation to vessels with this reconstruction (arrow). Setting a shortcut for MIPs in PACS is a great tool to quickly evaluate the vessels. 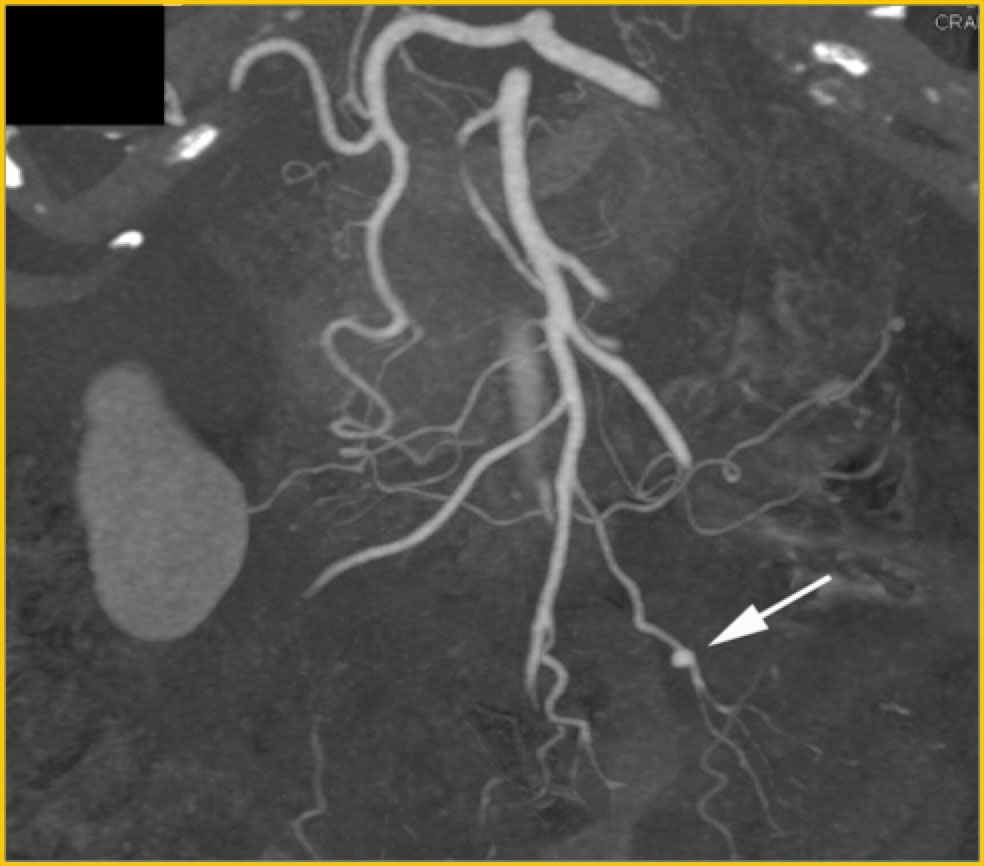 |
True Aneurysms: Celiac Artery Aneurysm 63-year-old man presenting with abdominal pain. Axial IV contrast enhanced CT (A) with incidental celiac artery fusiform aneurysms are noted and completely depicted in relation to vessels with 3D rendering (arrows) (B and C).3Ds are not necessary for diagnosis but helpful for non-radiologists. 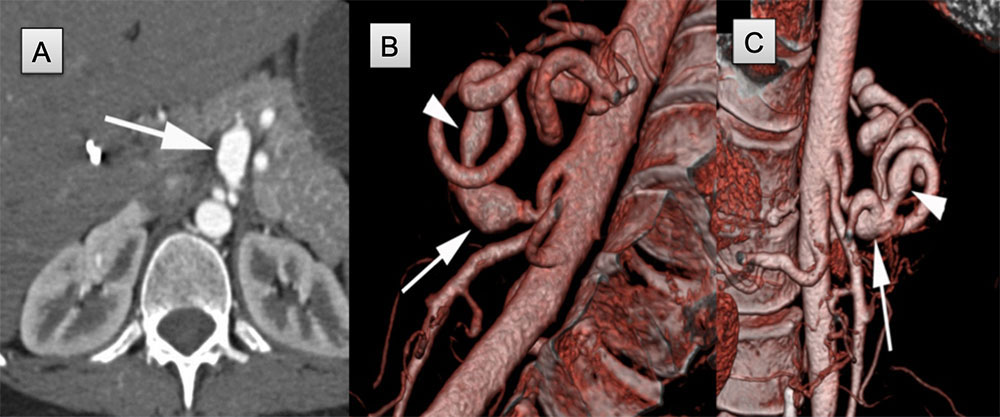 |
Celiac Artery Aneurysm Management
|
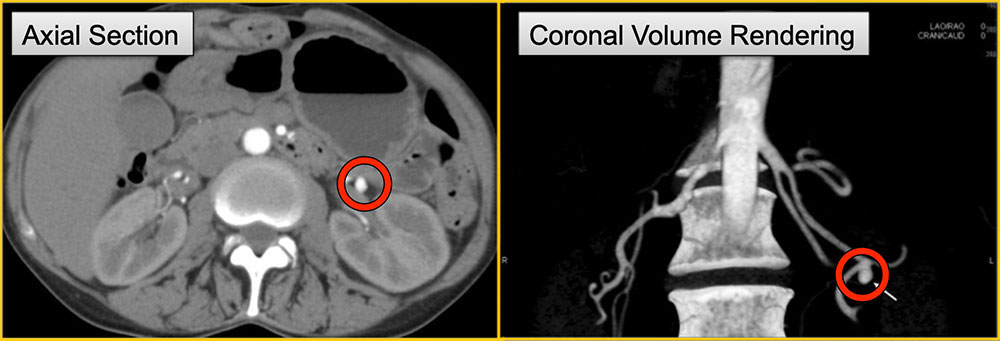
True Aneurysms: Gastroduodenal Artery Aneurysm 66 year old woman for routine follow-up of cholangiocarcinoma resection. IV contrast enhanced CT in axial (A), coronal (B) and coronal 3D rendering (C) demonstrating focal fusiform 8 mm of the GDA (arrows). 3D rendering best depicts the aneurysm. Note lack of surrounding hemorrhage or mural thrombus. 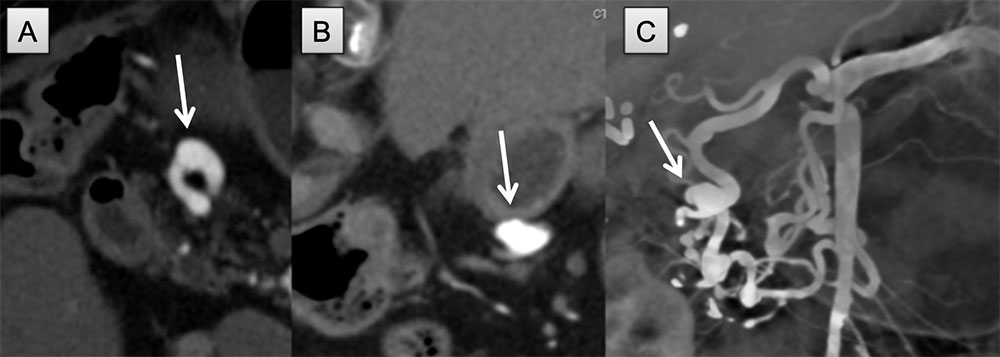 |
True Aneurysms: Renal Artery Aneurysm 61-year-old male with fever and pain at incision site of previous hip surgery. IV contrast enhanced CT of the abdomen in axial (A) and coronal (B) planes in arterial phase demonstrating 1.5 cm saccular aneurysm at main renal artery bifurcation (most common location). Note lack of surround hemorrhage or mural thrombus. 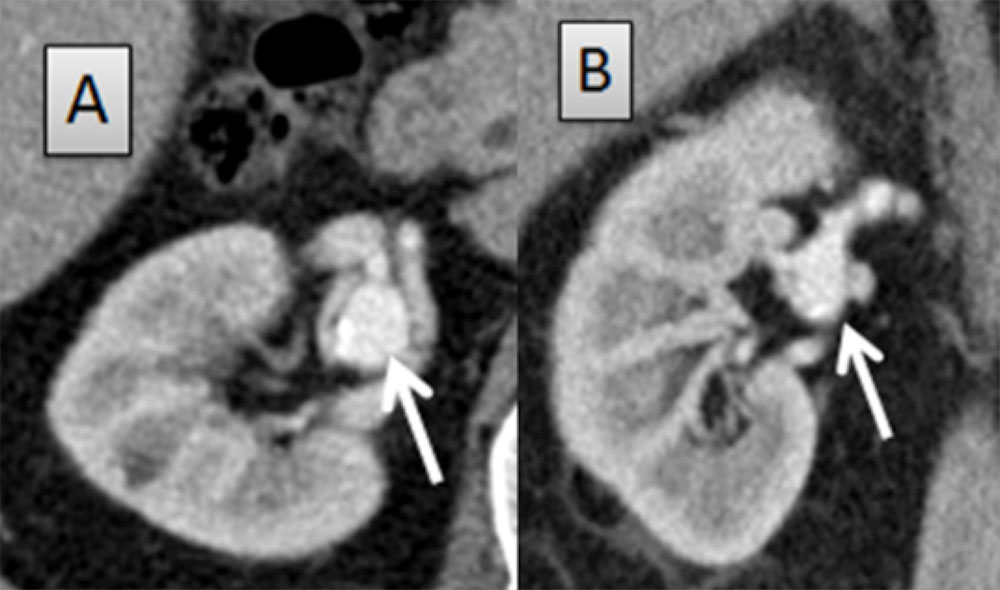 |
Visceral Arterial Aneurysms General Management
|
Pseudoaneurysms General
|
Splenic Artery Pseudoaneurysms Two patients. 45-year-old man with pancreatitis (A). Axial contrast enhanced CT demonstrates > 2 cm splenic pseudoaneurysm (red arrow) with an irregular wall surrounded by large amounts of hemorrhage (*). 18-year-old trauma patient (B). Axial contrast enhanced CT demonstrates 1 cm pseudoaneurysm (white arrow) surrounded by hemorrhage as well as splenic laceration (arrow head). 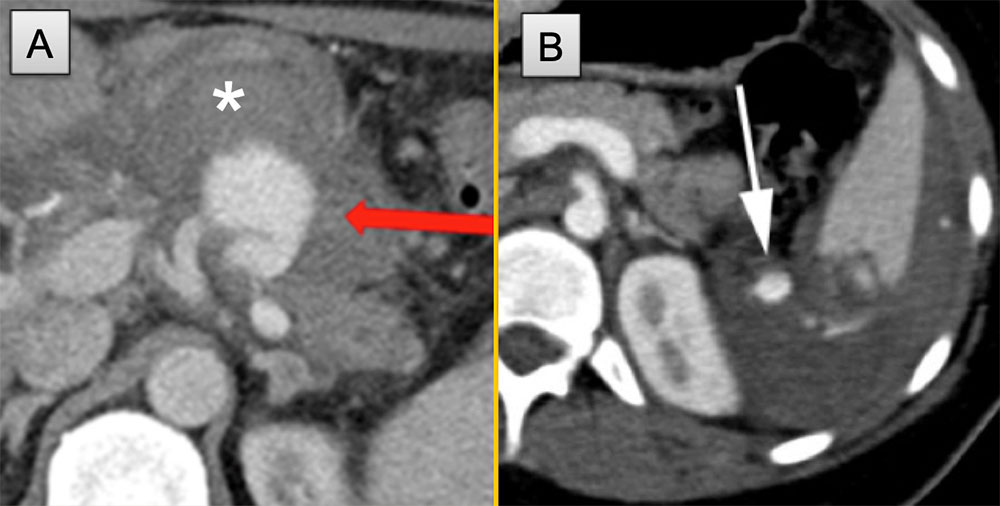 |
GDA Pseudoaneurysm 50 year old man with pancreatitis. IV contrast enhanced CT in coronal thin section (A) and MIP (B) demonstrates a 2 cm enhancing mass with a minimal hypodense halo, consistent with pseudoaneursym from a GDA/GDA branch in the pancreatic head (arrows). Incidental PV clot noted (arrowhead). 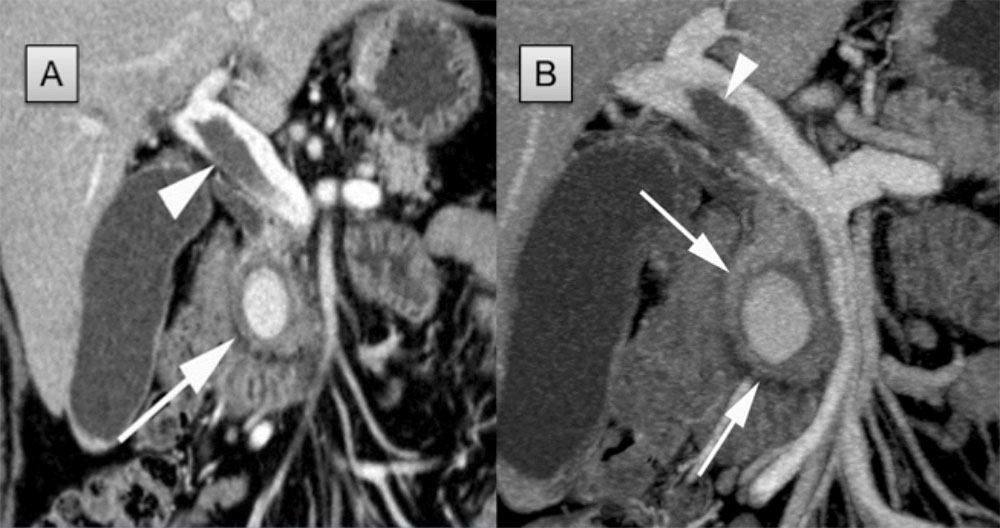 |
Hepatic Artery Pseudoaneurysm 69-year-old woman with pancreatic status post Whipple procedure. Postoperatively, Jackson Pratt drain had continued high output, which became serosanguinous. CT performed with axial image (A) and coronal MPR revealing a hepatic artery pseudoaneurysm. Trauma by any source, is by far the most common etiology for hepatic pseudoaneurysm formation. Note adjacent hemorrhage. 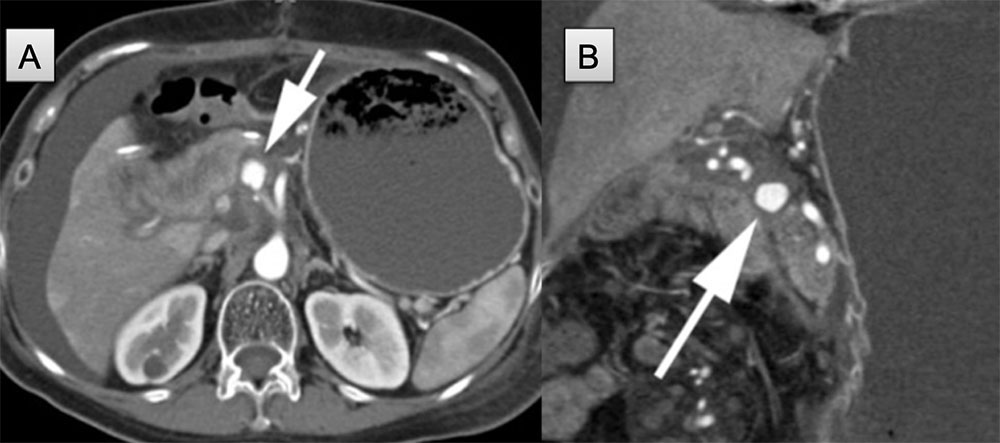 |
Renal Artery Pseudoaneurysm 57-year-old woman status post right robot assisted laparoscopic partial nephrectomy readmitted with abdominal pain and emesis. Coronal (A) and axial images (B) show a right perinephric hematoma and a large pseudoaneurysm (arrow) arising from lower pole renal artery. Note all the features of pseudoaneurysm formation: history, mural hemorrhage, and associated findings. 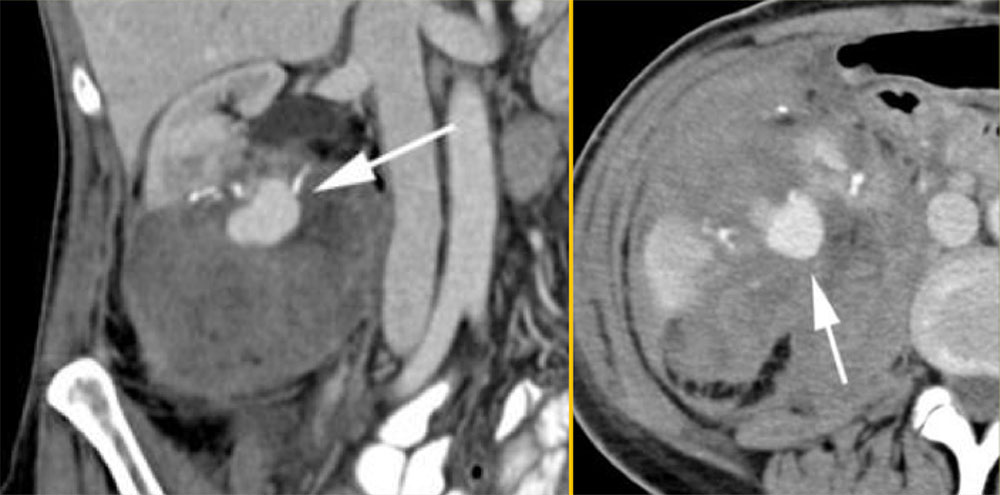 |
Coil Embolization of Renal Artery PSA 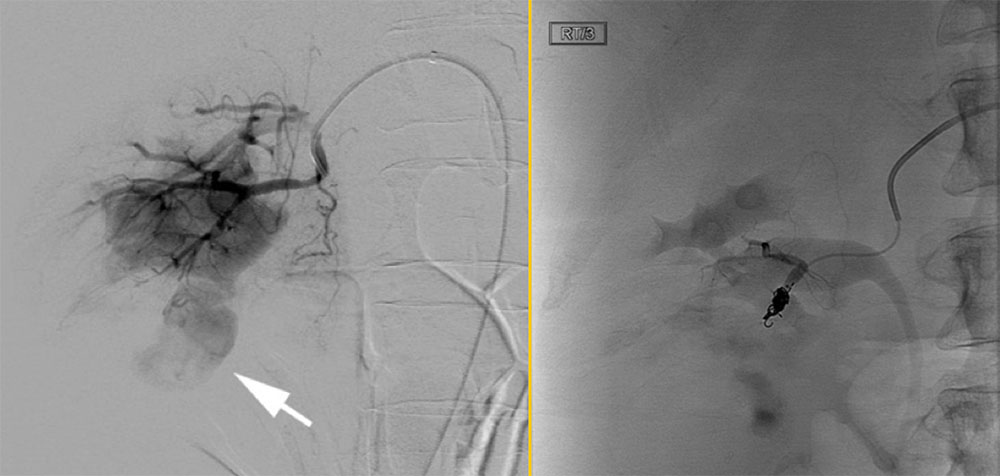 |
Conclusions
|
References
|