Computed Tomography of Aortic Arch Anatomy in Adults : Common and Unusual Variants
Computed Tomography of Aortic Arch Anatomy in Adults : Common and Unusual Variants EK Fishman, MD Johns Hopkins Hospital The Russell H. Morgan Department of Radiology and Radiological Science |
Simplified Late Stage Aortic Arch Development 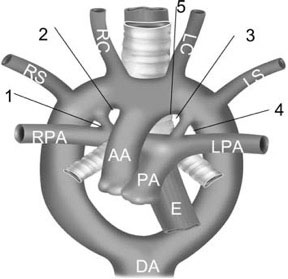 Model based on Edwards’ hypothetical double arch with bilateral ducti. Breaks at 1 and 2 lead to left arch Breaks at 3 and 4 lead to right arch. Break at 1, with resorption of the right ductus, results in normal anatomy. Break at 2 results in left arch with aberrant subclavian; typically the right ductus resorbs. Break at 4 results in right arch with mirror-image branching; the ductus runs from the innominate artery to the left pulmonary artery, and there is no ring. Break at 3 leads to right arch with aberrant subclavian; typically the left ductus persists, coursing from the descending aortic diverticulum to the left pulmonary artery, forming a common type of vascular ring. Break at 5 differs only in that the aberrant vessel is the innominate artery |
Normal Anatomy 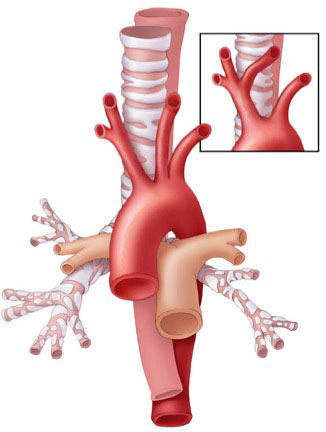
|
Vascular Ring Hierarchy
|
Left AA with aberrant right subclavian artery
|
Abberrant Right Subclavian Artery 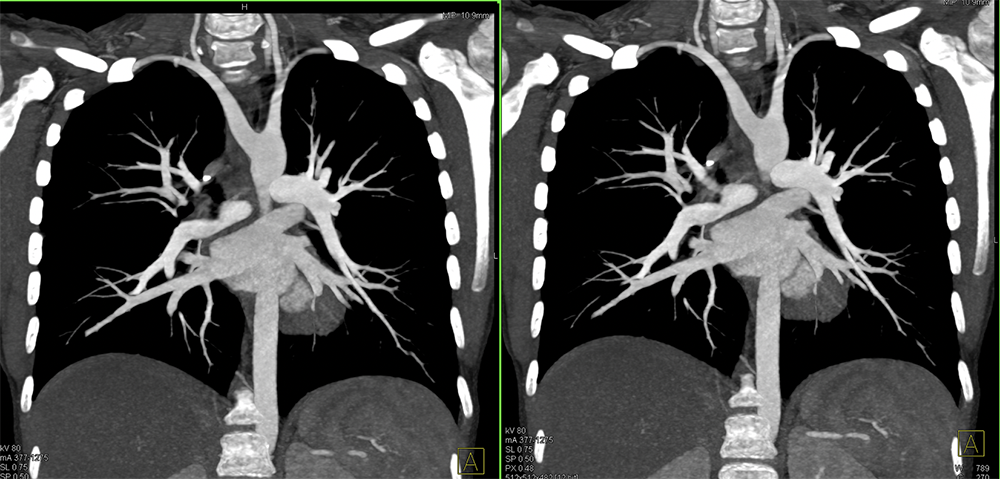 |
 |
Abberrant Right Subclavian Artery 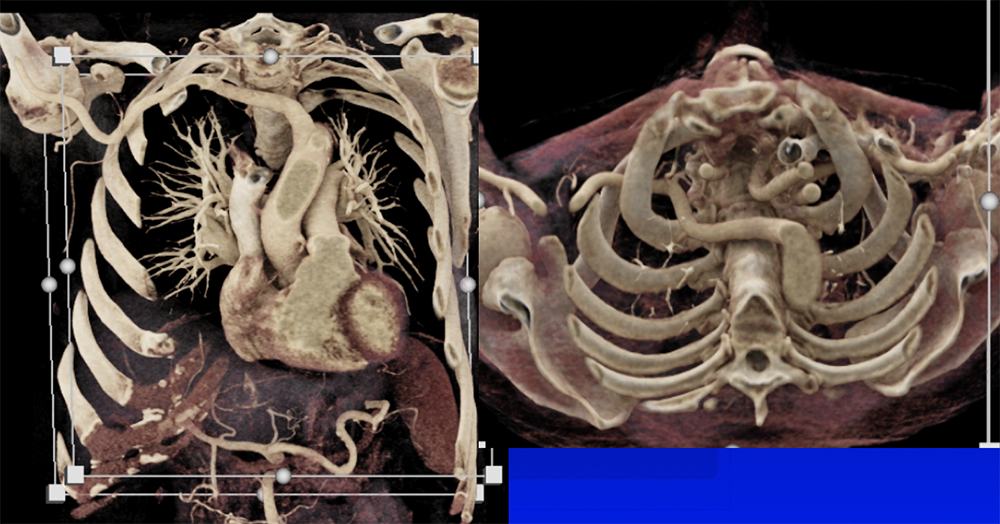 |
 |
 |
Right AA with aberrant left subclavian artery 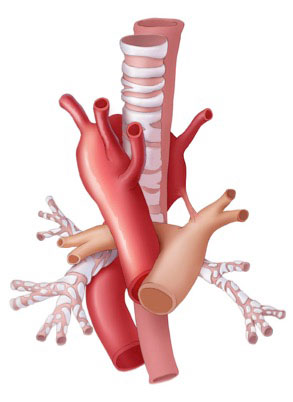
|
Right AA with mirror image branching 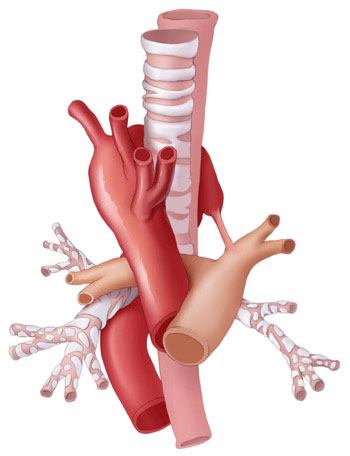
|
Double aortic arch 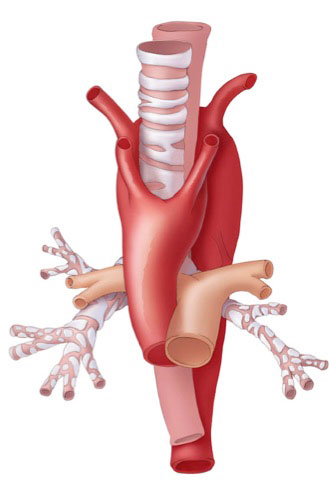
|
Hybrid lesion – CPAM type I and intralobar sequestration
|
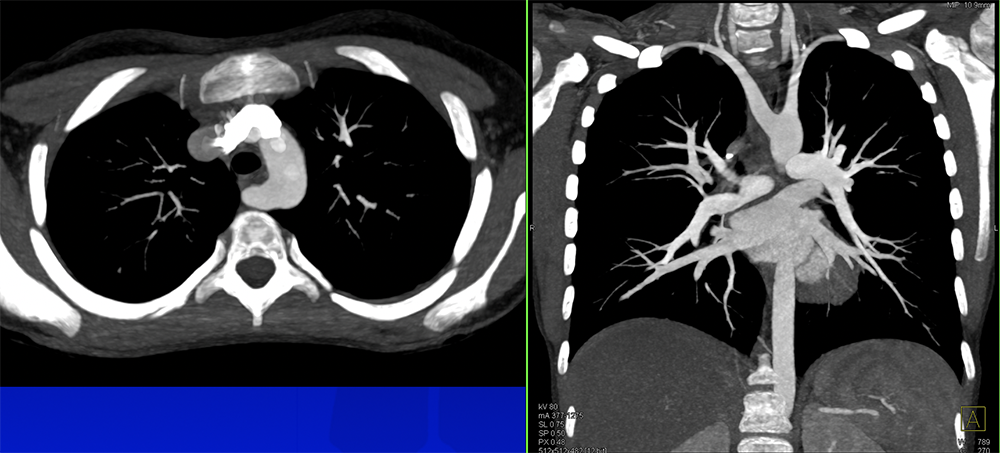
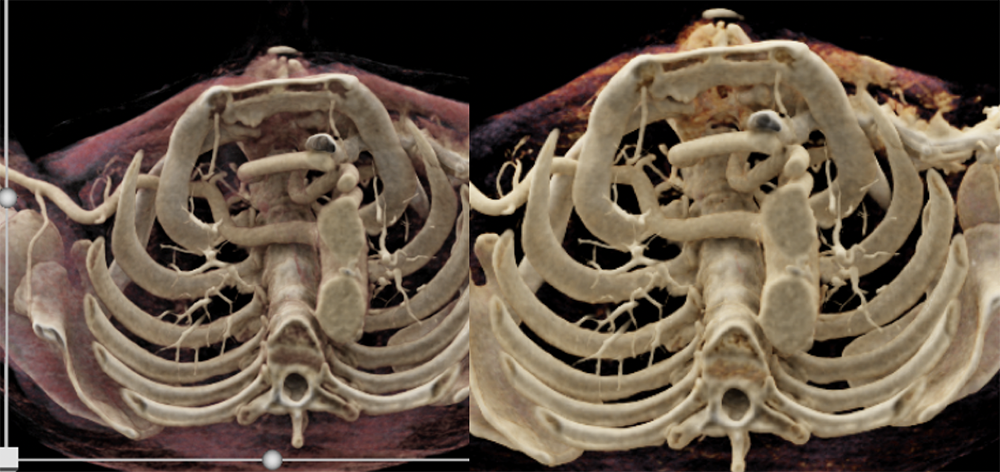
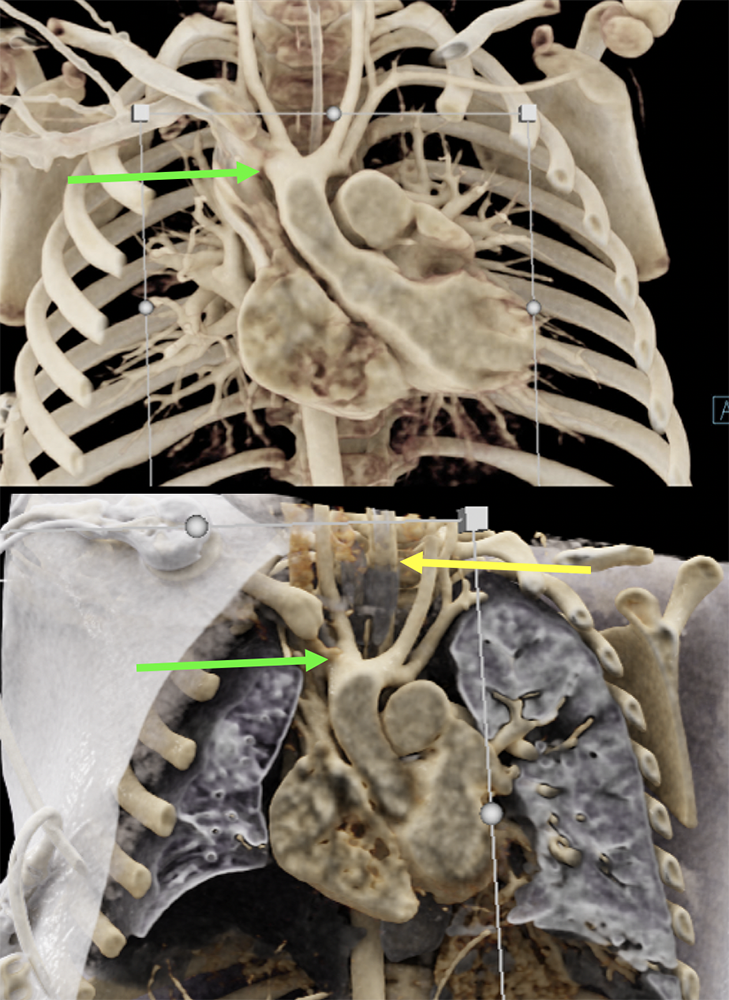 The coronal CR images demonstrate the double aortic arch, with a dominant right sided arch, which is the typical configuration. Both common carotid arteries and the left subclavian artery are well demonstrated, however the right subclavian artery is obscured by the overlapping clavicle. The lower CR image also highlights the pulmonary parenchyma and airways, and shows the trachea located posteriorly. |
Normal Anatomy 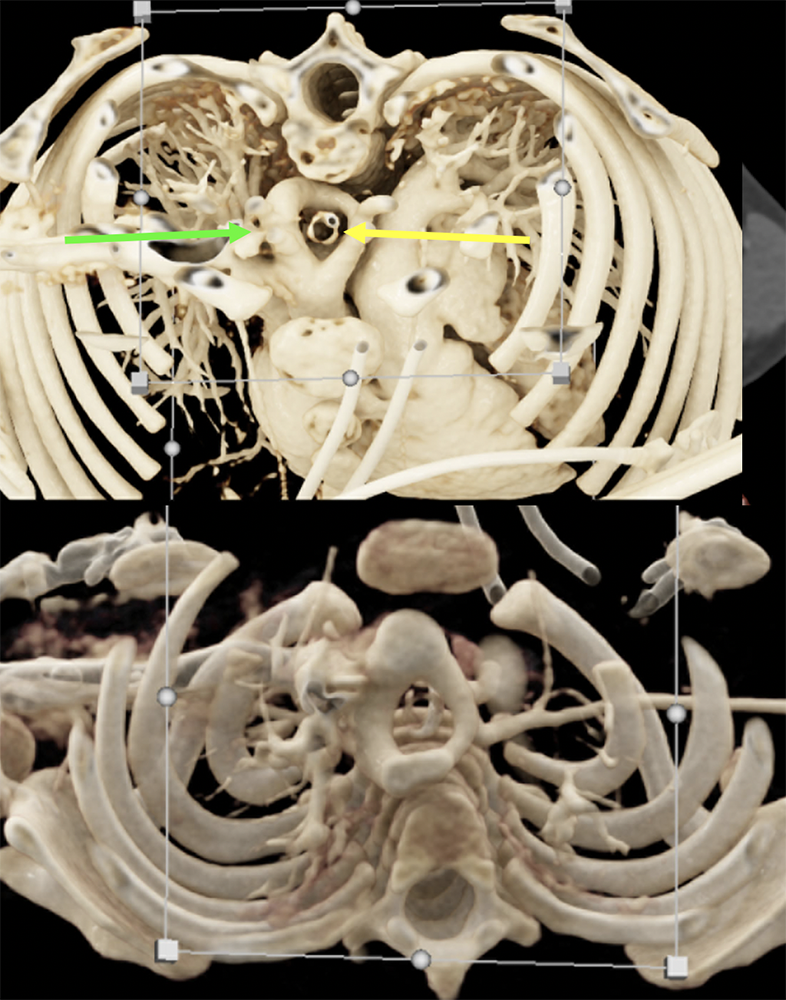 The complete vascular ring is demonstrated on both the standard MDCT image as well as the volume shape and me rendered image below. However the cinematic rendering provides even further anatomic detail of the vascular ring, and shows it completely encircling the endotracheal tube. The adjacent pulmonary vasculature and osseous structures are also well demonstrated. |
Normal Anatomy The coronal CR image highlights the double arch encircling the trachea posteriorly, as they are able to be isolated given the removal of the anterior aspects of the arch. The larger right arch is also nicely shown. The patient underwent surgical repair, with diversion of the non dominant left arch, division of the PDA ligament and aortopexy of the Kommerel diverticulum. |
References
|