The Role of CTA with 3D Mapping in the Evaluation of Vascular Stents beyond the Abdominal Aorta: Techniques, Interpretation, and Pitfalls
The Role of CTA with 3D Mapping in the Evaluation of Vascular Stents beyond the Abdominal Aorta: Techniques, Interpretation, and Pitfalls Johns Hopkins Hospital Department of Radiology |
Introduction
|
Complications of Stent Placement
|
Technique: Data Interpretation
|
Interactive 2D and 3D Rendering 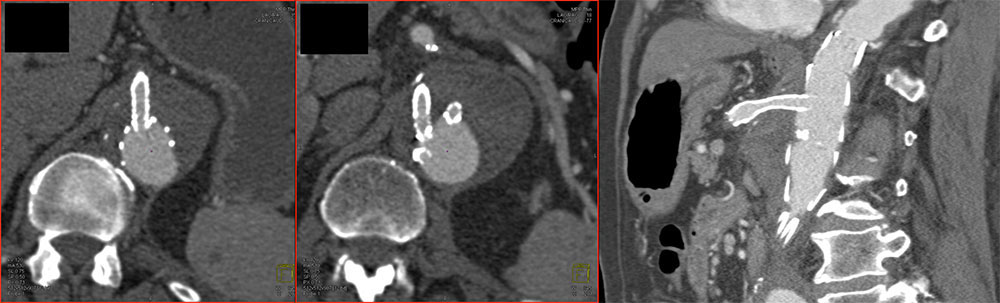 Axial images and 2D MPRs perpendicular to long axis of stent to evaluate stent lumen |
Interactive 2D and 3D Rendering 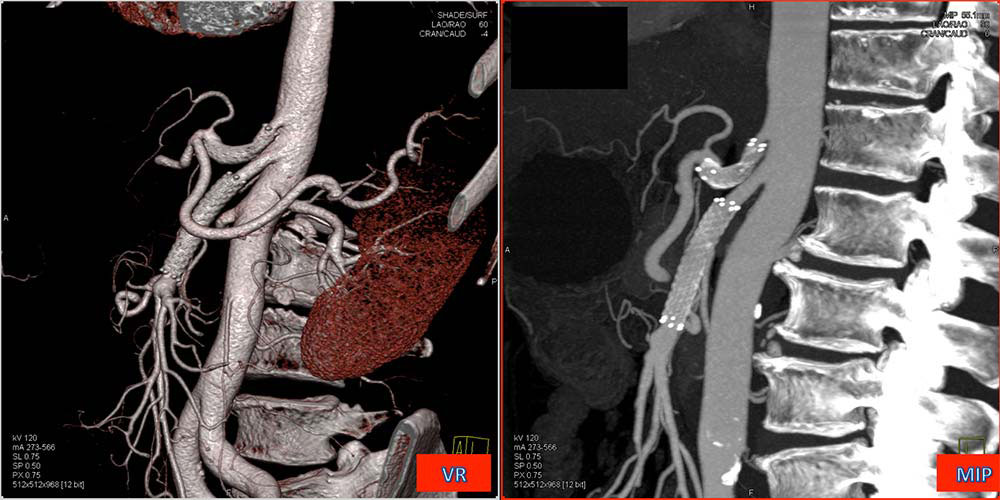 VR (volume rendering) and MIP (maximum intensity projection) to create vascular map and show distal vessel patency. Volume rendering conveys 3D relationships and is best for evaluation of end organs because tissue density is maintained; MIP is better for small branch visualization. |
Indications
|
Mesenteric Ischemia
|
Mesenteric Ischemia
|
SMA Stenosis 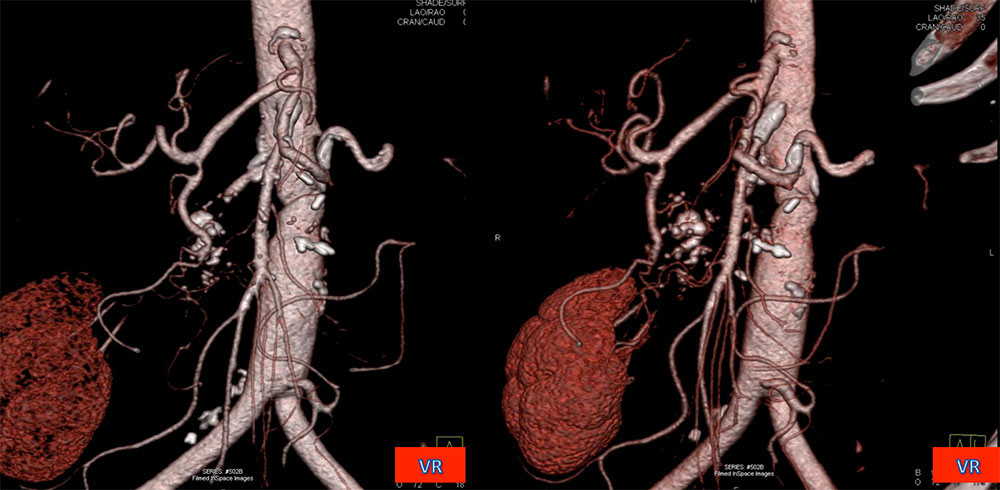 66 year old woman, long standing smoker with severe atherosclerotic disease s/p aortobifemoral bypass and stenting of SMA for stenosis. Coronal and coronal oblique color coded volume renderings show show stent in the proximal SMA with patency of the distal vessel. |
SMA Stenosis 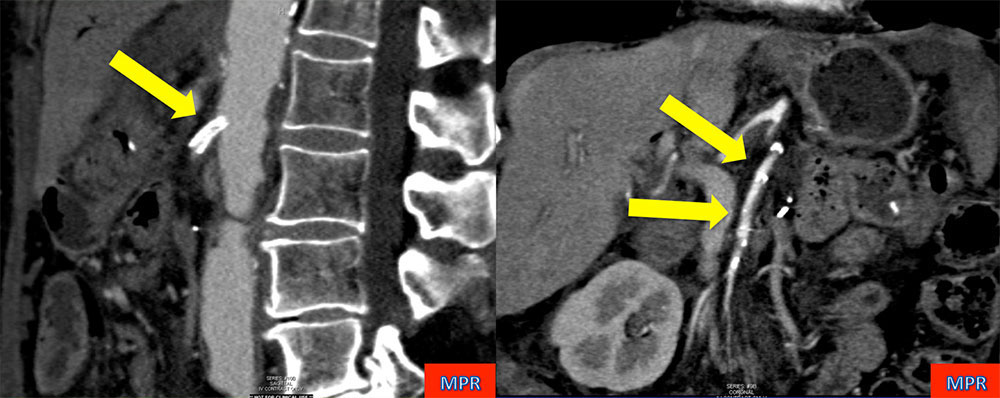 66 year old woman, long standing smoker with severe atherosclerotic disease s/p aortobifemoral bypass and stenting of SMA for stenosis. Sagittal and coronal MPRs show stent in the proximal SMA with patency of the distal vessel. |
Mesenteric Ischemia: Stent Occlusion  45 year old woman with history of chronic mesenteric ischemia secondary to multiple vascular occlusions, s/p multiple arterial stents (celiac artery, proximal and distal SMA) shown with coronal and sagittal VR, which provide a nice overview of the anatomy. |
Occluded SMA Stent 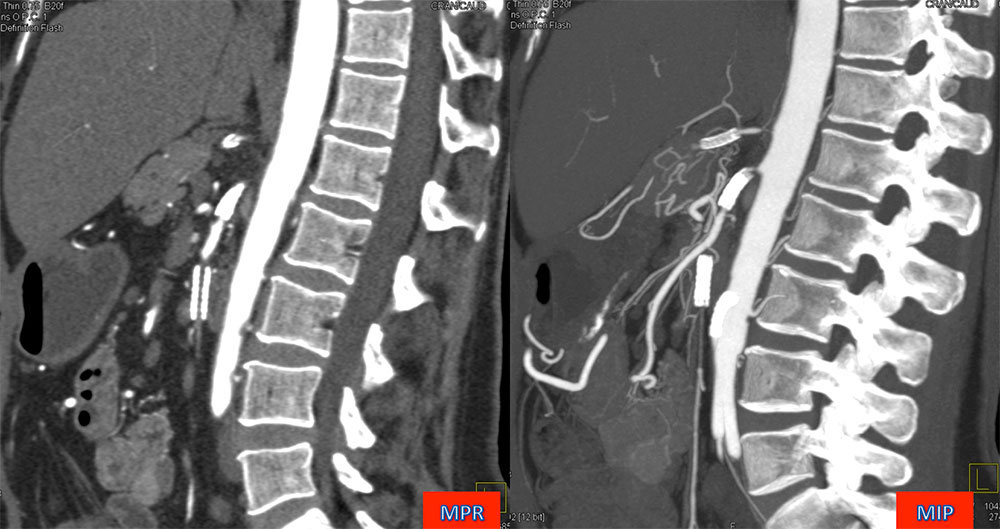 45 year old woman with history of chronic mesenteric ischemia secondary to multiple vascular occlusions, s/p multiple arterial stents. Sagittal MPR and MIP demonstrate the thrombosed lumen of the inferior SMA stent and absence of enhancement in the artery distal to the stent. |
Chronic Mesenteric Ischemia Other Causes
|
Celiac Artery Stent for MALS 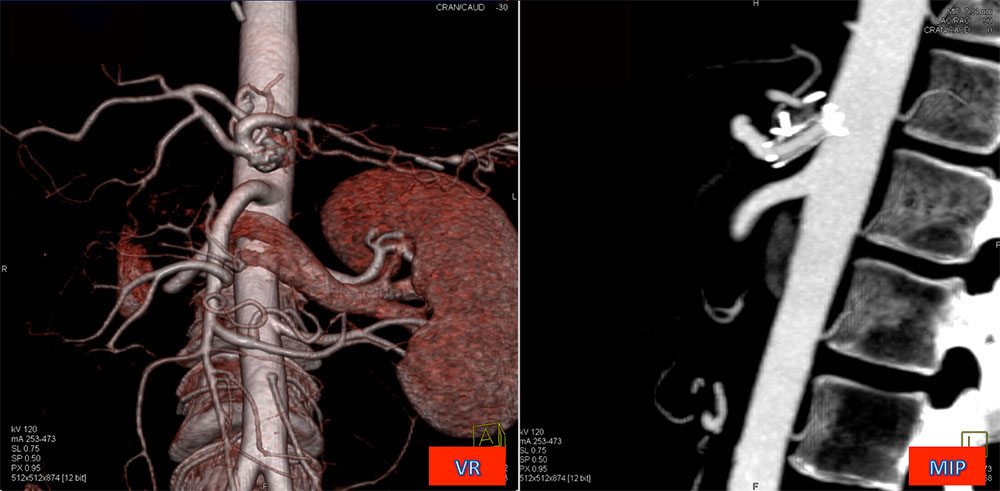 46 year old woman with long history of postprandial abdominal pain who underwent division of median arcuate ligament and celiac artery stent placement. Coronal color coded volume rendering shows patent celiac axis. Modification of the rendering parameters and application of a clip plane with a sagittal MIP rendering document patency of the stent lumen. |
Celiac Artery Stent for MALS 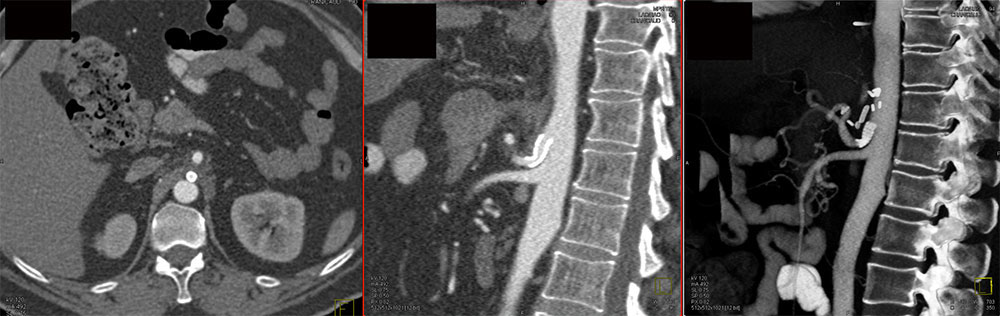 43 year old man with median arcuate ligament syndrome s/p surgical repair with celiac artery stent. Axial image shows stent, but patency best demonstrated by sagittal MPR through the lumen and sagittal volume rendering to show distal vessel perfusion. |
Visceral Arterial Aneurysms
|
Visceral Arterial Aneurysms
|
Splenic Artery Aneurysm  62 year old woman with splenic artery aneurysm s/p attempted stent placement complicated by splenic artery dissection. Coronal volume renderings in various obliquities show persistent aneurysm of the splenic artery despite presence of stent. |
Mesenteric Artery Dissection 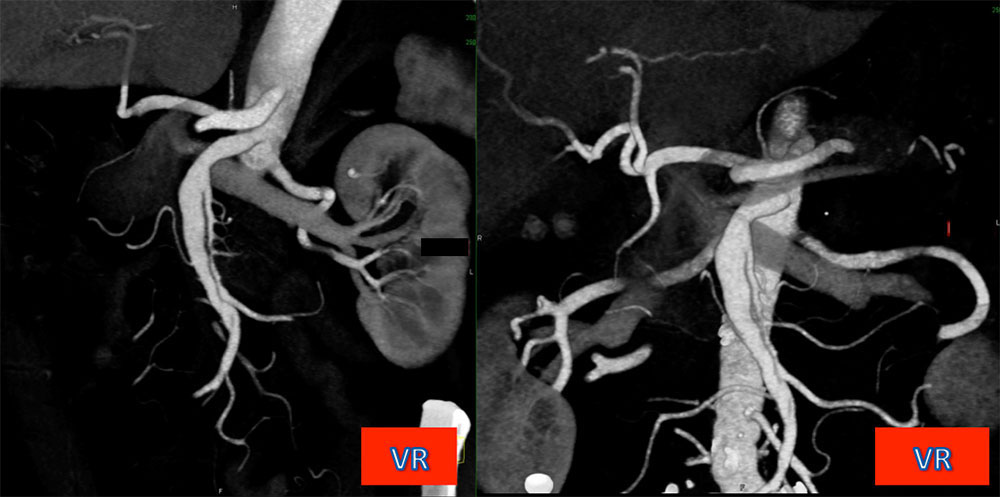
|
SMA Dissection 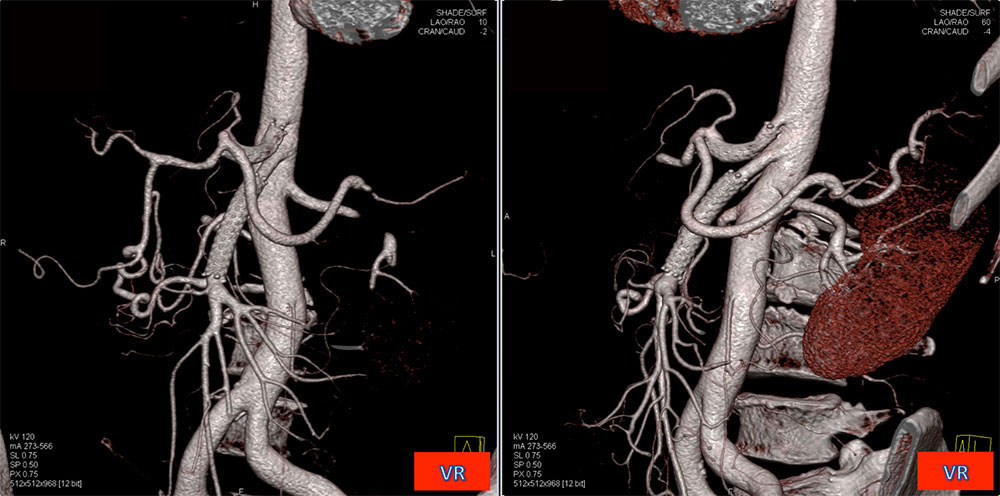 66 year old man with marfanoid connective tissue disorder presented with acute abdominal pain. Diagnosed with SMA dissection and underwent stent placement in SMA and celiac arteries. Coronal and coronal oblique color coded volume renderings nicely map patent celiac artery and SMA following stent placement. |
SMA Dissection 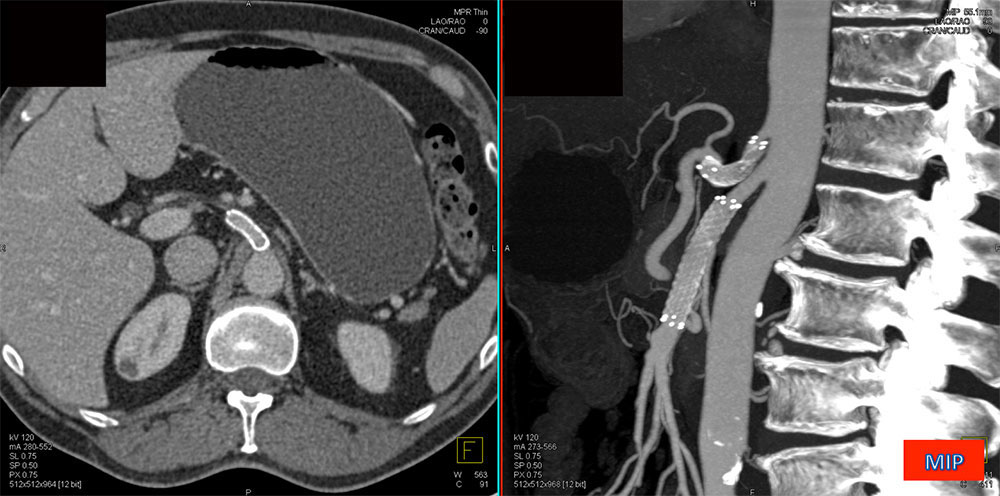 66 year old man with marfanoid connective tissue disorder who presented with acute abdominal pain. Diagnosed with SMA dissection and underwent stent placement in SMA and celiac arteries. Stent patency confirmed by axial image through the lumen and vascular mapping with sagittal MIP, demonstrating perfusion distal to the stents. |
Renal Artery Stenosis
|
RAS: Benefits of Stenting
|
Renal Artery Stenosis 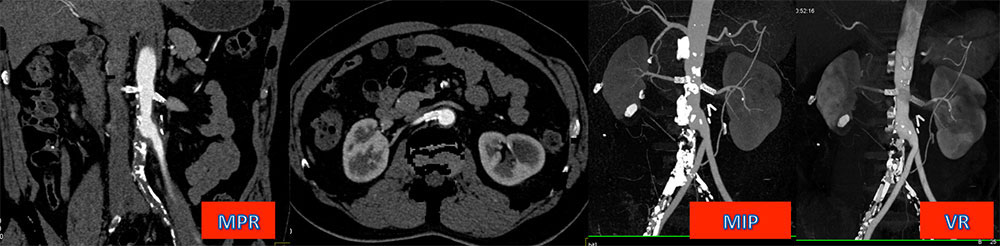 63 year old man s/p infrarenal abdominal aortic repair and bilateral renal artery stents for renovascular hypertension. Axial CT and coronal MPR show perfused stent lumen. Coronal MIP and volume rendering depict aortoiliac graft, patent renal arteries and symmetric renal enhancement in a single image. |
Renal Artery Aneurysms
|
Renal Artery Aneurysm 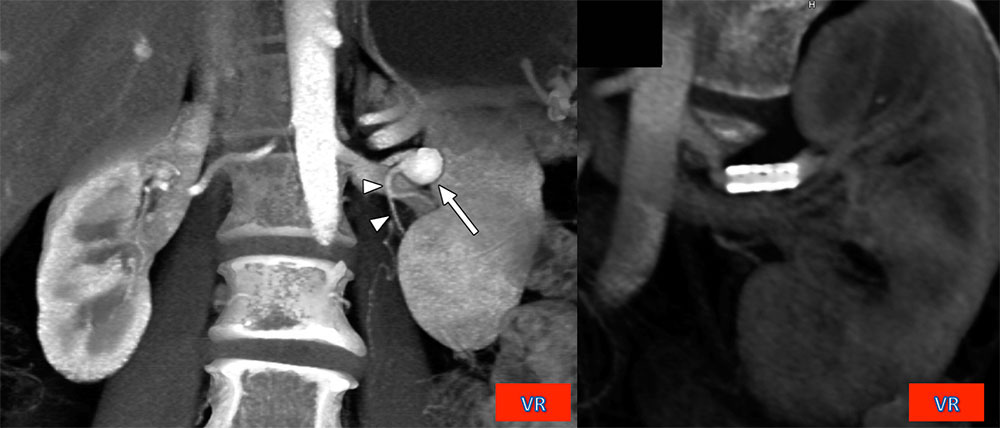 59-year-old woman with left renal artery aneurysm, treated by endoluminal stent placement. Coronal volume renderings shows aneurysm (left) and stent patency after intervention (right) by applying a clip plane to visualize the lumen. ©2010 by American Roentgen Ray Society, Johnson P T et al. AJR 2010;194:1001-1012 |
Aortic Aneurysm
|
Aortic Aneurysm 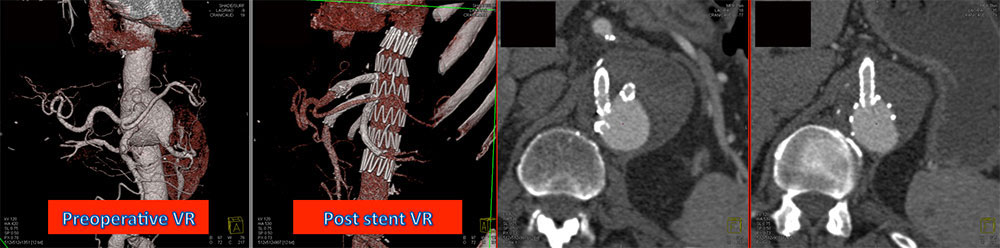 77 year old man with 6.5 cm infrarenal abdominal aortic aneurysm involving branch vessels. Repair included individual stent placement in celiac, SMA and renal arteries. Color coded volume rendering provides overview and shows patent distal vessels. Stent lumen patency demonstrated with axial images. |
Endoluminal Aortic Repair and Renal Artery Compromise 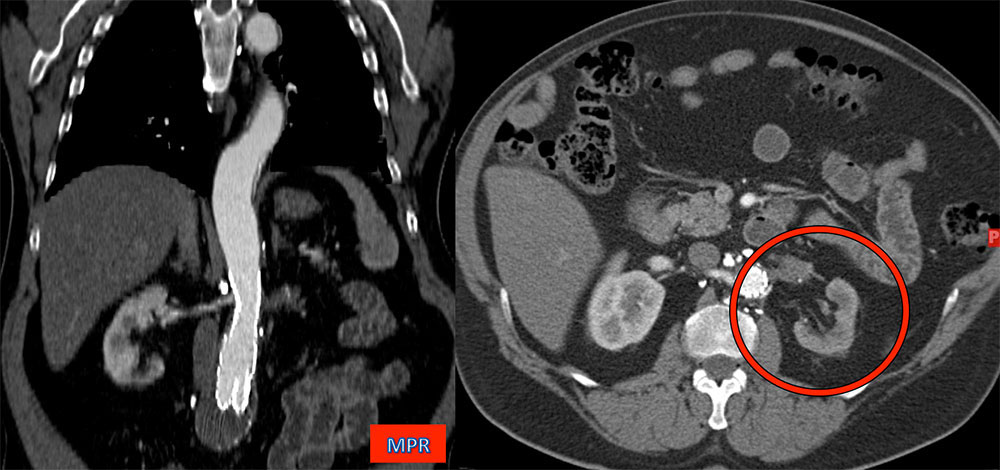 Left kidney perfusion compromised by aortic endoluminal stent crossing renal artery orifice. Diminished renal enhancement shown on axial image (ring). |
Endoluminal Aortic Repair and Renal Artery Compromise 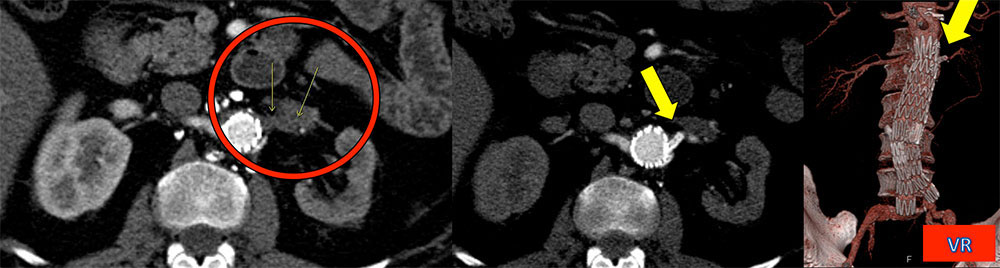 Left renal artery compromise (ring) treated with left renal artery stent (arrow), which restored perfusion to the left kidney. |
Conclusion
|
References
P T Johnson, MD K M Horton, MD E K Fishman, MD |