Calcified Pancreatic Lesions: Differential DxCalcified Pancreatic Lesions: Differential Dx |
Overview of Calcified Pancreatic Lesions  |
Pancreatic Neuroendocrine Tumor
|
Pancreatic Neuroendocrine Tumor 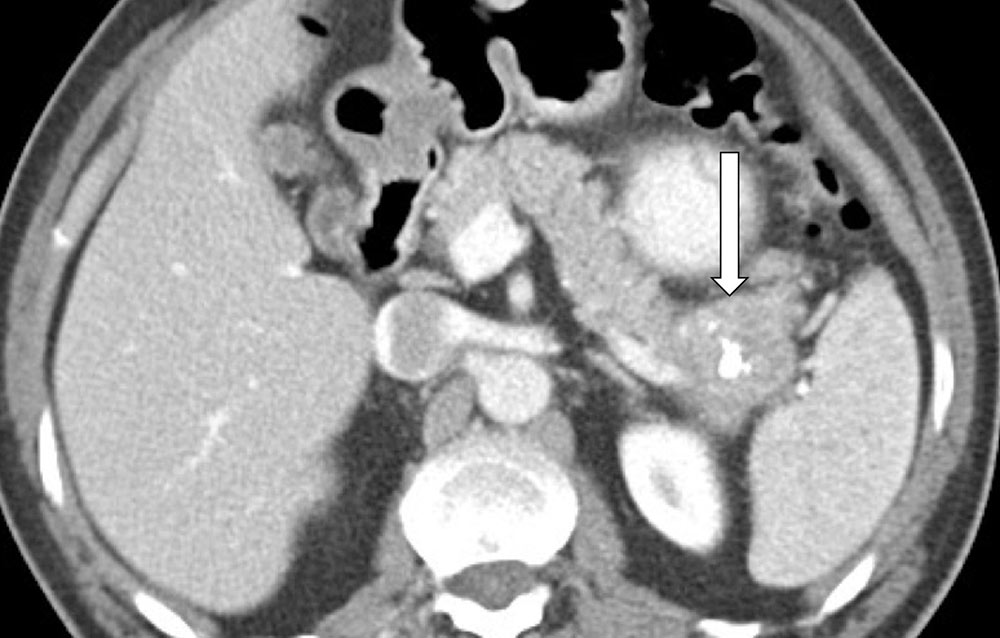 |
Pancreatic Neuroendocrine Tumor Multiple gastrinomas with calcification resulting in severe gastric wall thickening due to Zollinger-Ellison syndrome 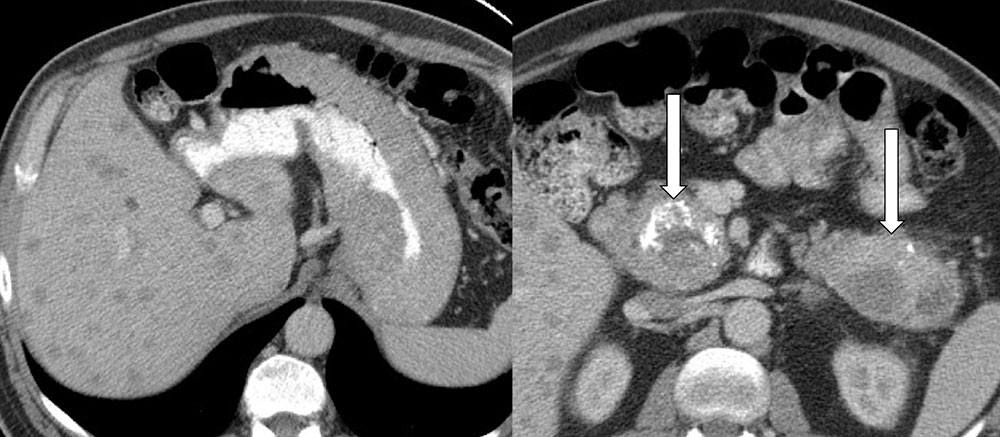 |
Serous Cystadenoma
|
Serous Cystadenoma 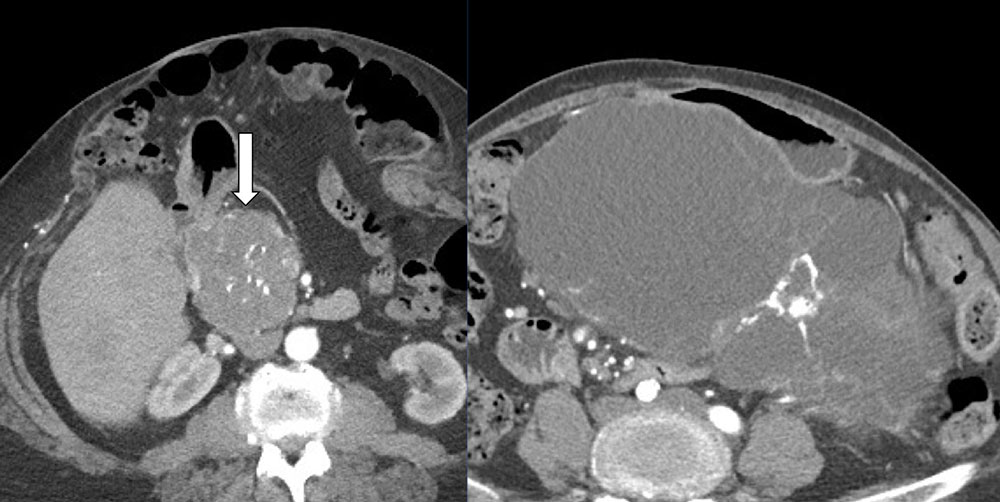 |
Serous Cystadenoma Subtle internal calcification in a serous cystadenoma with honeycomb or ‘sponge’ pattern  |
Serous Cystadenoma As in this case, calcifications in serous cystadenoma are often located at the center of the lesion in the vicinity of the central scar  |
Mucinous Cystic Neoplasm
|
Mucinous Cystic Neoplasm Calcification in mucinous cystic neoplasms (MCN) tend to be peripheral, thin, and curvilinear.  |
Mucinous Cystic Neoplasm Note the presence of subtle peripheral curvilinear calcification at the margin of this MCN. The location of the lesion, the age and gender of the patient, and the pattern of calcification should allow a confident, specific diagnosis.  |
Solid and Pseudopapillary Neoplasm
|
Solid and Pseudopapillary Neoplasm SPEN tumors very commonly demonstrate calcification, perhaps dystrophic in nature related to the frequent intralesional hemorrhage present within these lesions. 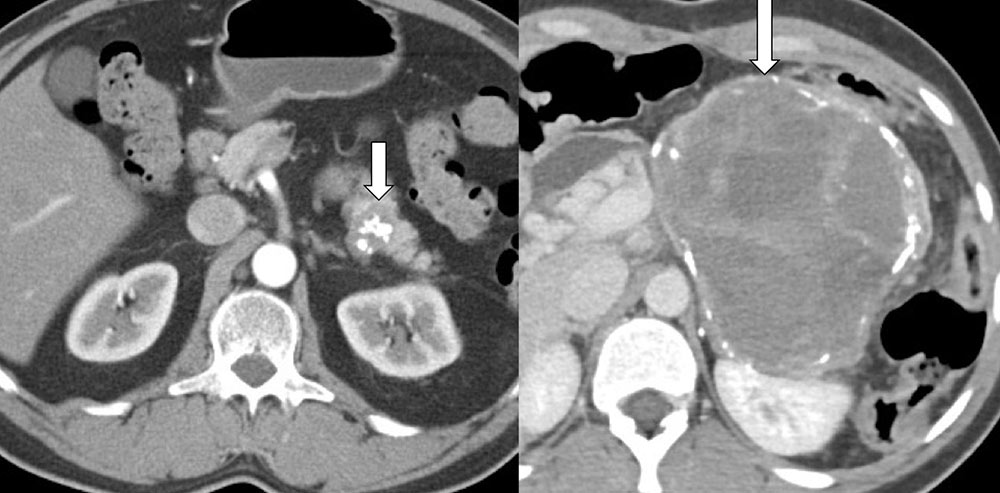 |
Solid and Pseudopapillary Neoplasm 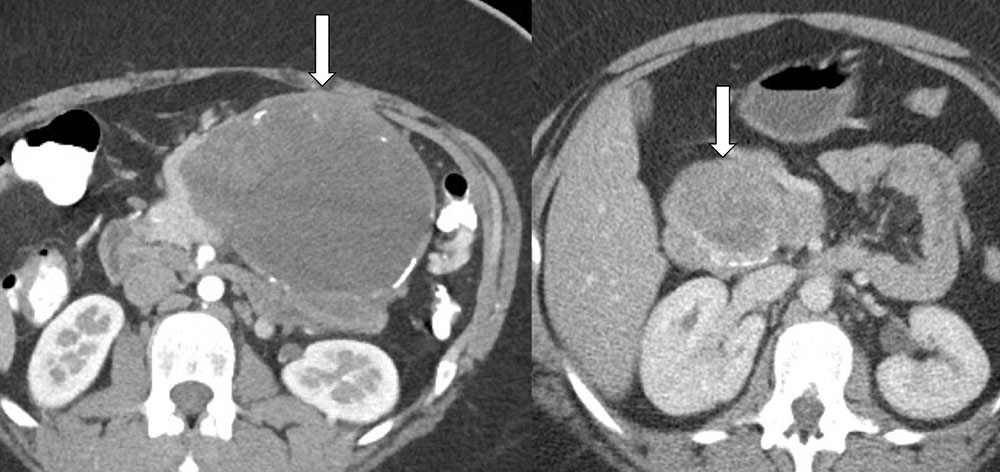 |
Intraductal Papillary Mucinous Neoplasm (IPMN)
|
Intraductal Papillary Mucinous Neoplasm (IPMN) Side-branch IPMN are reported to calcify in ~20%, although our own experience suggests (anecdotally) that calcification is relatively uncommon in IPMN 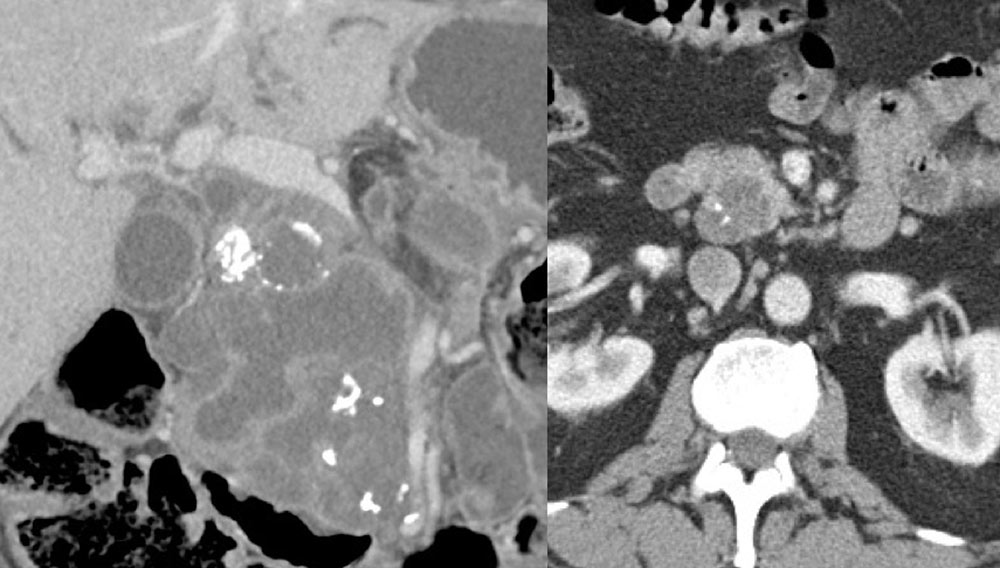 |
Intraductal Papillary Mucinous Neoplasm (IPMN) Main-duct IPMN with markedly dilated pancreatic duct containing amorphous calcifications. While described as a common feature in the literature, our own experience is that this is a relatively rare imaging pattern.  |
Other Solid or Cystic Pancreatic Masses
|
Pancreatic Pseudocyst  |
Pancreatic Metastasis Beautiful example of a mucinous colon cancer metastasis to the pancreas with internal stippled calcifications  |
Which pancreatic mass does not calcify? Conventional pancreatic adenocarcinoma virtually never demonstrates calcification, with the exception of rare pancreatic mucinous adenocarcinomas Unusual pancreatic mucinous adenocarcinoma with internal calcification 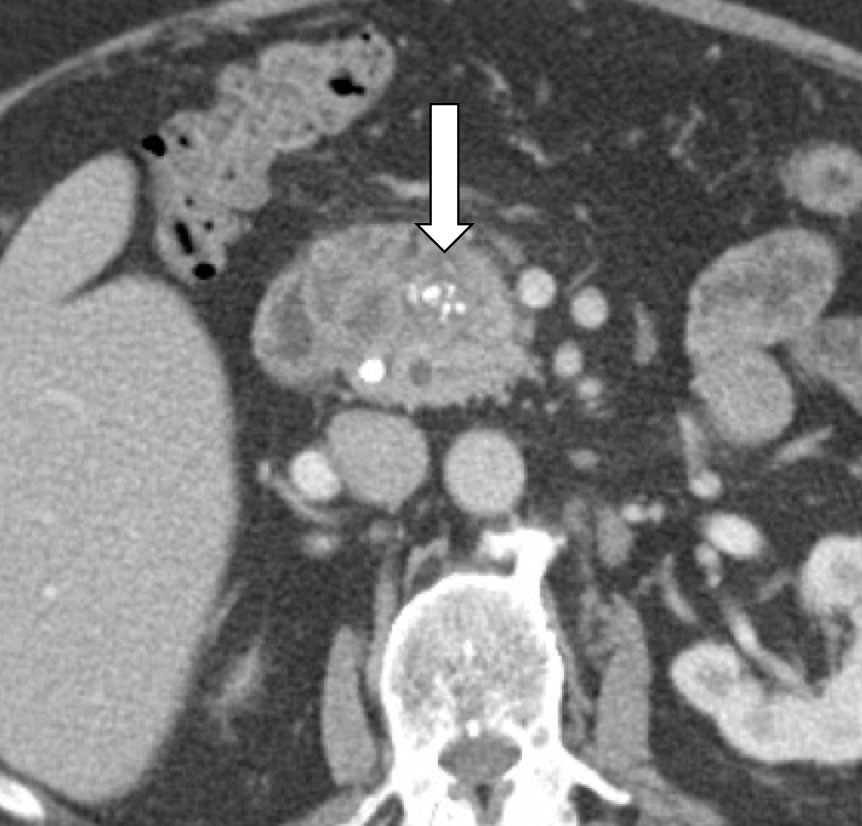 |
Chronic Pancreatitis
|
Chronic Pancreatitis Focal calcified mass in the pancreatic head in patient with chronic pancreatitis. As mentioned previously, the presence of calcification within this mass argues strongly against the possibility of pancreatic adenocarcinoma  |
Mimics of Primary Pancreatic Calcifications
|
Conclusion
|
References
|