State-of-the-art Diagnosis and Treatment of Metastatic Melanoma: MDCT Protocol Optimization to Identify Metastases in Unusual Locations and Review of Innovative Therapeutic AgentsState-of-the-art Diagnosis and Treatment of Metastatic Melanoma: MDCT Protocol Optimization to Identify Metastases in Unusual Locations and Review of Innovative Therapeutic Agents Elliot K. Fishman, M.D. The Russell H. Morgan Department of Radiology and Radiological Science The Johns Hopkins Medical Institutions Baltimore, Maryland |
Cardiac Metastasis 62-year-old man with melanoma metastatic to the right ventricle. Axial IV contrast enhanced CT with soft tissue (A) and high contrast (B) windows. Tumor conspicuity is enhanced by use of high contrast window (B). 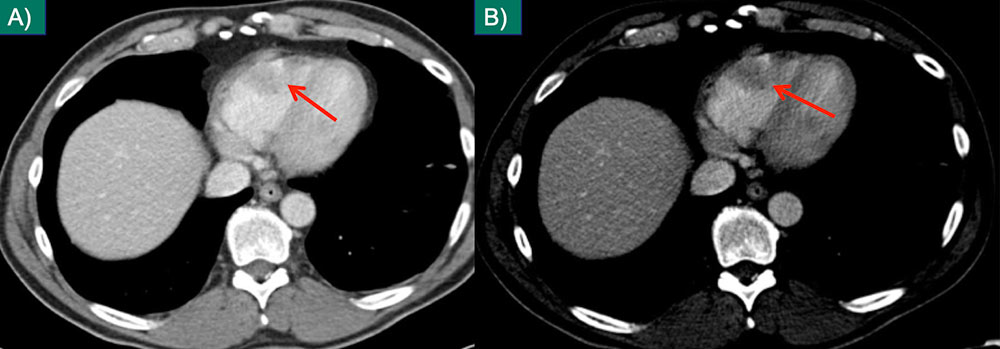 |
Intramuscular Metastases 55-year-old female with melanoma. Intramuscular metastasis (A) better visualized with high contrast window (B) in axial plane. Second muscular metastasis in the same patient on standard axial soft tissue window (C) and coronal MPR with contrast window (D). 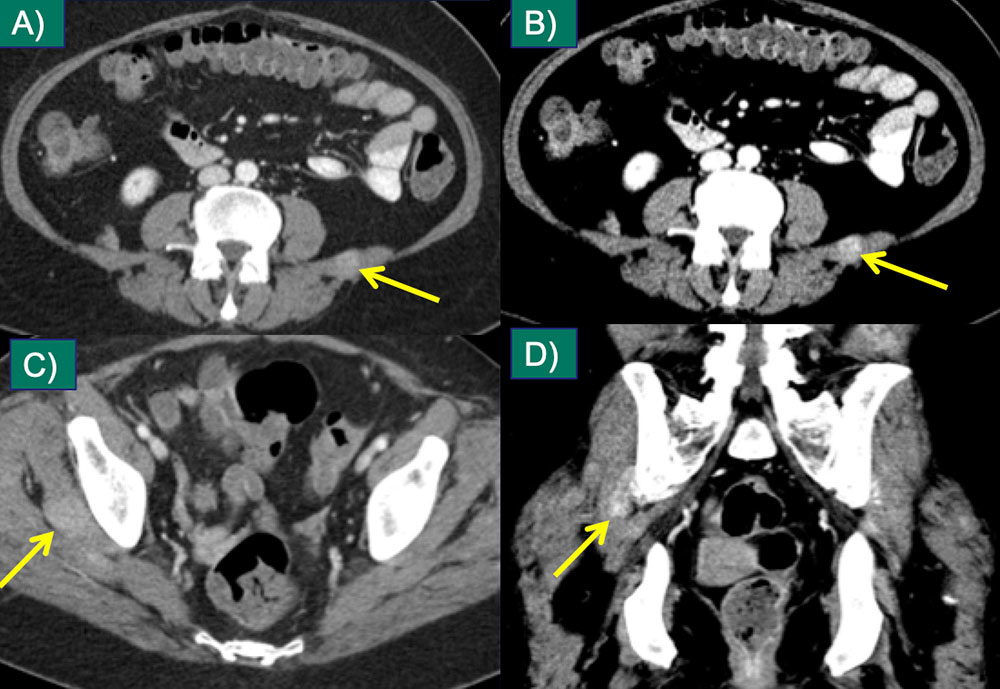 |
Spinal Canal 76-year-old male with melanoma; soft tissue infiltration in the sacral spinal canal (A) is better appreciated on the sagittal MPR with a soft tissue window (B), which also reveals cortical erosion of the posterior sacrum (C). 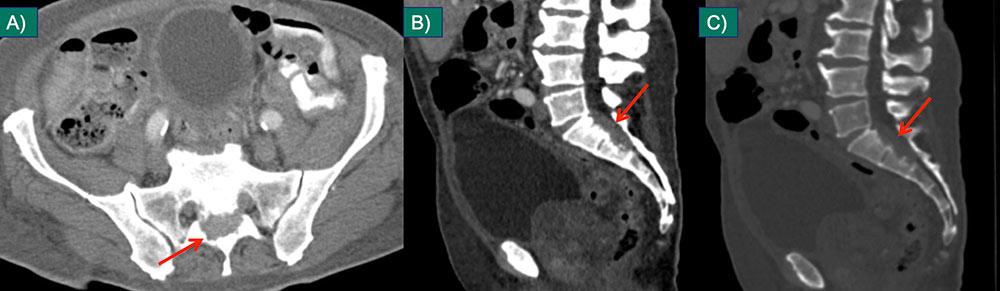 |
Parotid Metastasis 48-year old woman with melanoma and enhancing mass in the left parotid on axial (A) and coronal (B) IV contrast-enhanced CT. Metastases to solid organs are best visualized with high contrast windows (B). Confirmation with coronal MPR increases diagnostic confidence. 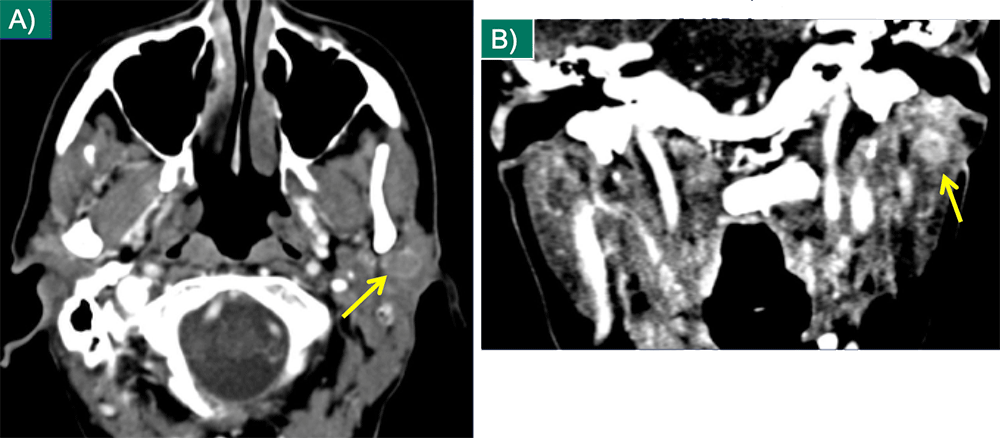 |
Thyroid Metastasis 55-year-old female with melanoma and thyroid metastasis seen on axial (A) and coronal (B) IV contrast-enhanced CT.  |
Pancreatic Metastasis 65-year-old woman with pancreatic mass due to metastatic melanoma. Axial image (A) and coronal MPR (B) from IV contrast enhanced CT show a hypovascular mass in the pancreatic body with ductal dilation in the distal body and tail. The metastasis mimics a primary pancreatic adenocarcinoma. 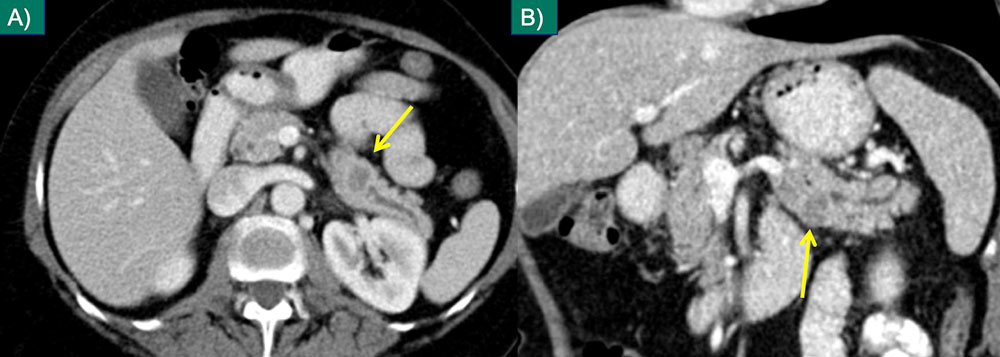 |
Small Bowel 56-year-old man with multifocal small bowel wall thickening due to metastatic melanoma involving both the jejunum (A) and ileum (B) on coronal IV contrast enhanced CT. Note that this appearance mimics lymphoma involving small bowel. 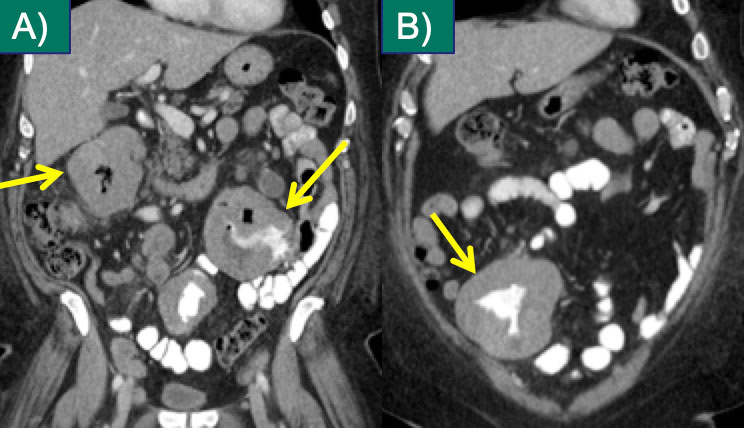 |
Small Bowel 78-year-old man with melanoma and nodular metastatic lesions in the small bowel wall on axial (C) and coronal (D) IV contrast enhanced CT. Small bowel should be inspected on axial and coronal planes to identify small metastases. 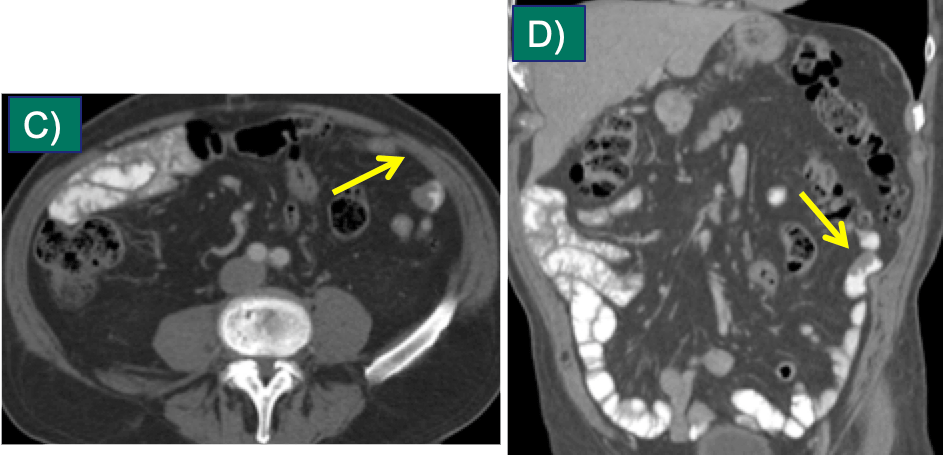 |
Mesenteric Metastasis 66-year-old man with melanoma and new mesenteric nodule on axial (A) and coronal (B) IV contrast enhanced CT. Coronal MPRs facilitate distinction of mesenteric metastases from bowel. Note intense FDG activity (C) on correlate PET image. 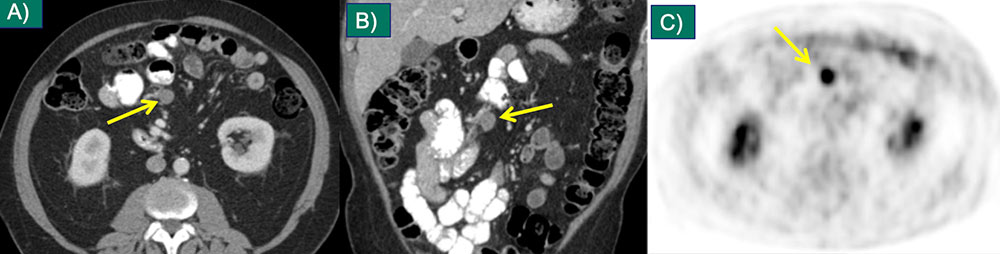 |
Perinephric Metastasis 55-year-old female with melanoma and small perinephric metastases on axial (A) and coronal (B) IV contrast-enhanced CT, which enlarged at 3 month follow up (C,D). (Same patient as slide 17) 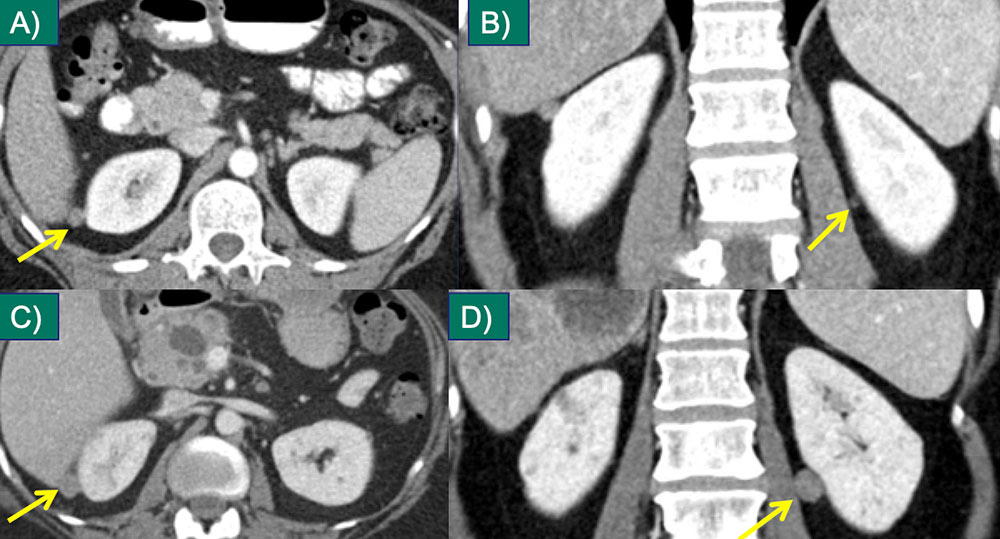 |
Uterine Metastasis 44-year-old female with melanoma and small uterine/periuterine nodule seen on axial IV contrast-enhanced CT (A). Intense FDG activity noted on follow-up PET/CT (B). No clear CT correlate (C) for a second focus of intense FDG activity in the uterus (D). PET/CT can identify some solid organ metastases not visualized with CT. 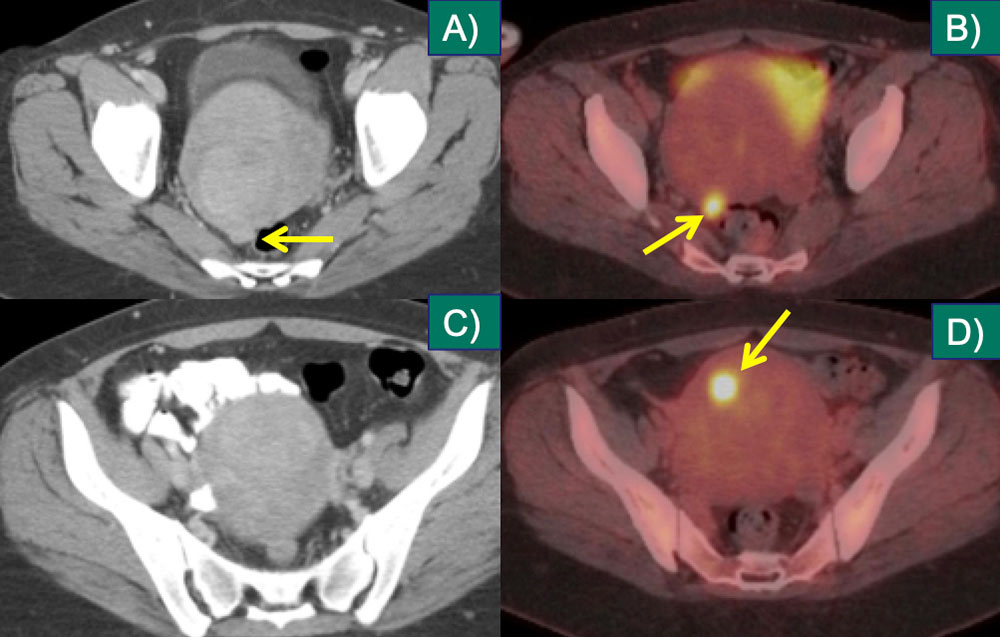 |
Cutaneous/Subcutaneous 56-year-old man with metastatic melanoma from right gluteal primary. Axial extended-field-of-view CT image demonstrates two skin metastases. Lower extremity, back, and head and neck melanoma metastasize to subcutaneous tissues.8 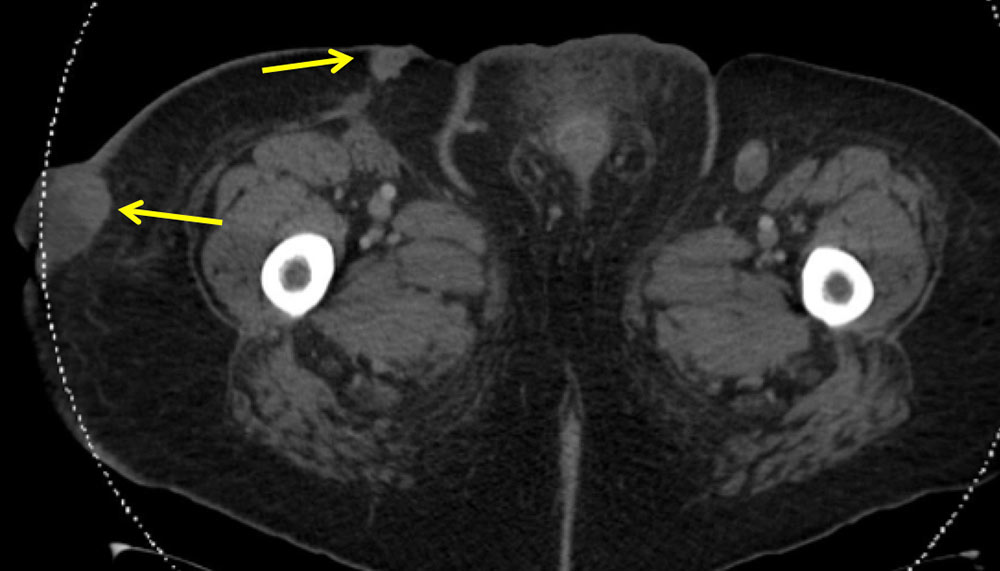 |
Isolated Subcutaneous Metastasis 51-year old woman with melanoma and small subcutaneous nodule that increased from 4 mm (A) to 8 mm (B). Note FDG avidity on PET/CT (C). This was the only site of metastatic disease. Careful inspection of the subcutaneous tissues with comparison to prior exams is imperative; subcutaneous metastases are often small at presentation. 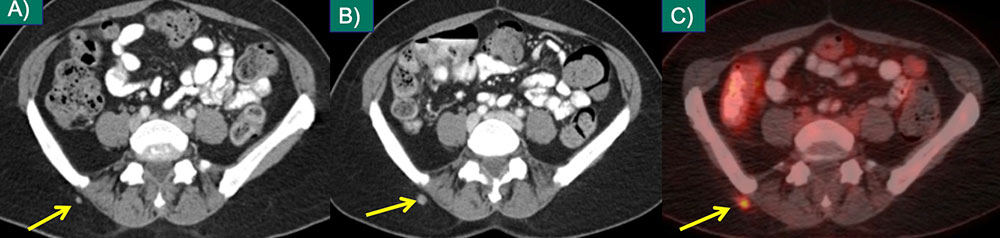 |
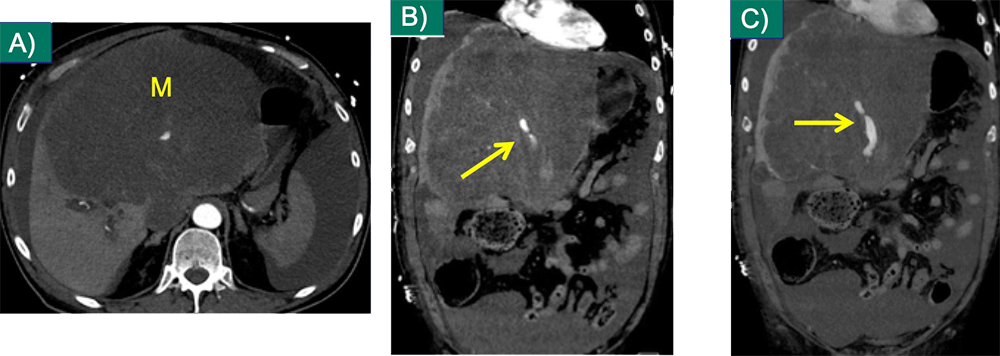
Complications of Melanoma Mets 57-year-old male with metastatic (M) to liver lesion on axial CT (A) and active hemorrhage on IV contrast enhanced MDCT arterial (B) and venous (C) phase coronal MPRS.
 |
On the Treatment Horizon Adoptive cell transfer:
|
Immunotherapy Complications Axial (A,B), sagittal (C), and coronal (D) IV and oral contrast enhanced CT demonstrating diffuse colonic wall thickening in a 68-year-old female on ipilimumab for therapy of metastatic melanoma. Severe colitis was found on subsequent colonoscopy: pathologic changes consistent with ipilimumab-related disease. 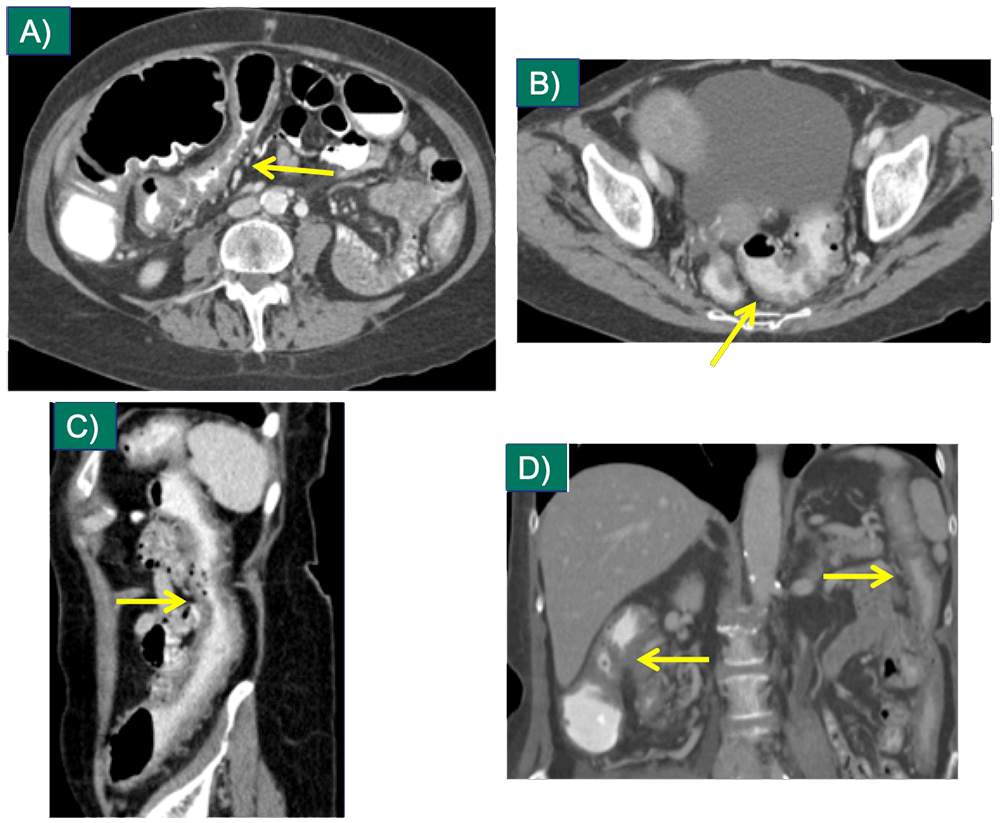 |
Immunotherapy Complications Axial non-contrast CT of the chest in lung windows (A,B) demonstrating consolidation in the left lung, consistent with pneumonitis in a patient who had received 4 doses of ipilimumab for therapy of melanoma. 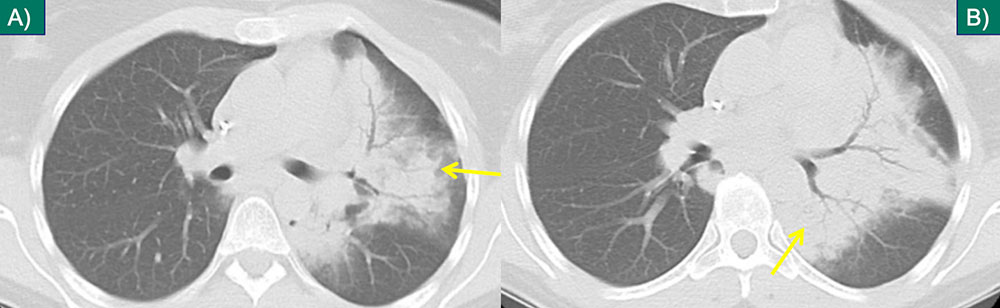 |
Immunotherapy Complications Axial (A-C) IV contrast-enhanced CT in a 68-year-old male with metastatic melanoma on ipilimumab presenting with abdominal pain and elevated lipase, with pancreatic edema and adjacent inflammatory stranding, compatible with acute pancreatitis. 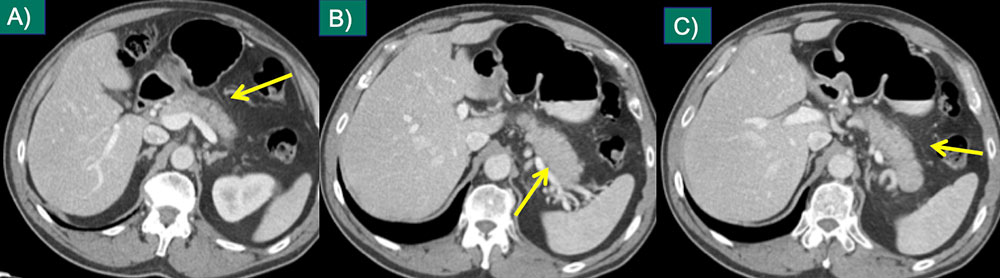 |
References
|