Postoperative Thoracic Aorta in the Marfan Patient: Normal Postoperative Appearance and Spectrum of Complications
Postoperative Thoracic Aorta in the Marfan Patient: Normal Postoperative Appearance and Spectrum of Complications |
Introduction
|
Marfan syndrome
|
Marfan Syndrome
|
Marfan Syndrome Cardiovascular manifestations
|
Dilated Aortic Root 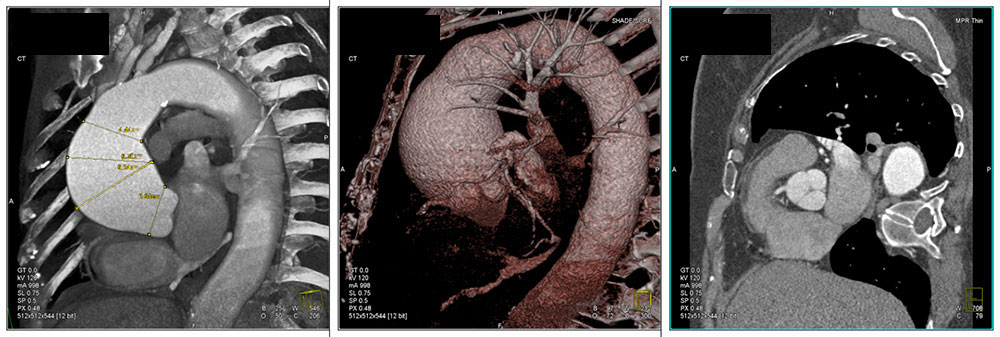 68 year old female with no history of surgical repair. 3D maps and reformatted images show dilatation of the supravalvular aortic root and ascending aorta characteristic of annuloaortic ectasia. Operative repair is indicated when aorta reaches a diameter of 5 cm due to high risk of rupture. Classic “tulip bulb” configuration. |
Cardiovascular manifestations
|
Post-operative complications
|
Case Studies
|
Case 1: Normal postoperative appearance in patient with composite graft and mechanical aortic valve replacement 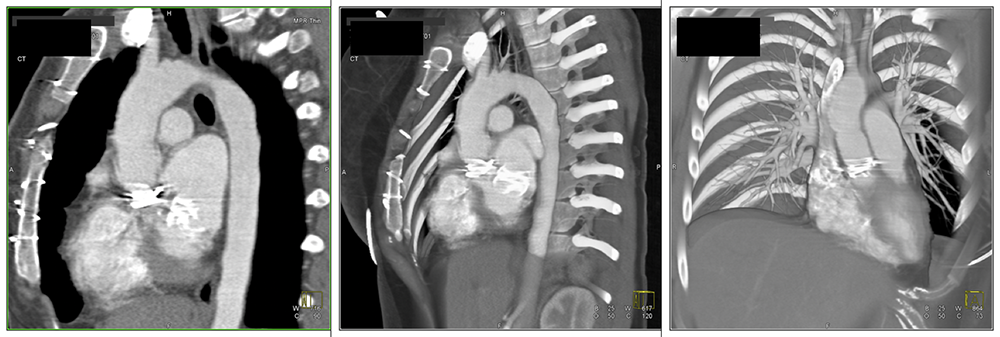 19 year old female presented for routine follow up evaluation. She has had prior aortic root replacement with composite graft as well as aortic and mitral valve replacement. Images A and B are sagittal reformations demonstrating artifact related to prosthetic aortic and mitral valves. Image C best shows the “waisting” of the ascending aorta due to composite graft placement. |
Case 2: Normal postoperative appearance in patient with valve-sparing operation 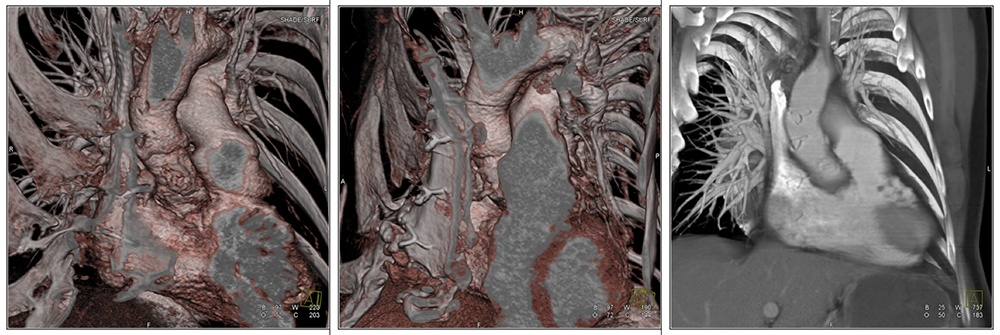 40 year old male with prior valve-sparing aortic root replacement. No complications seen. Note absence of valve replacement. The 3D maps (images A and B) best demonstrate the contour defect related to surgical repair and area of coronary artery re-implantation into the graft. Image C shows suture lines related to vascular graft. |
Case 3: Normal postoperative appearance in patient with valve-sparing operation 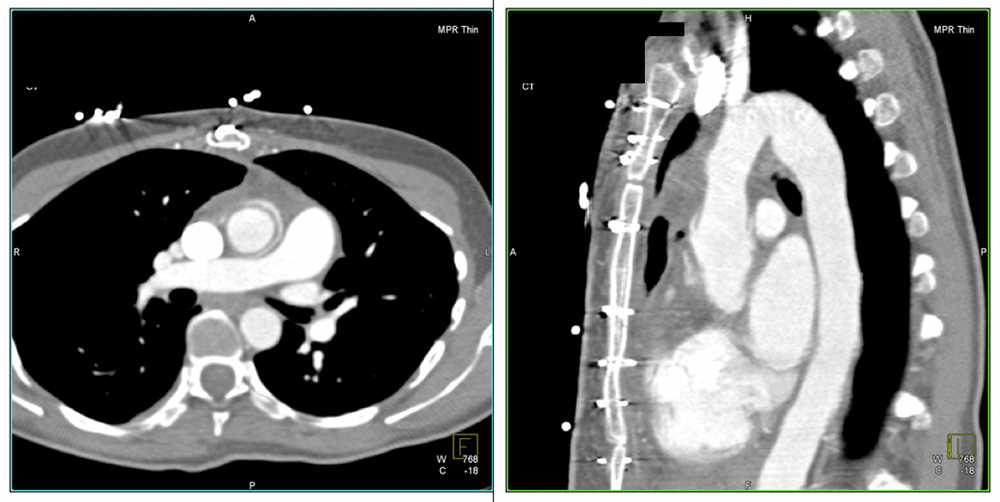 36 year old female with prior valve-sparing aortic root replacement. No complications seen. Axial and sagittal reformatted images demonstrate placement of vascular graft within the native aortic root and ascending aorta. Note absence of aortic valve replacement. |
Case 3: Normal postoperative appearance in patient with valve-sparing operation 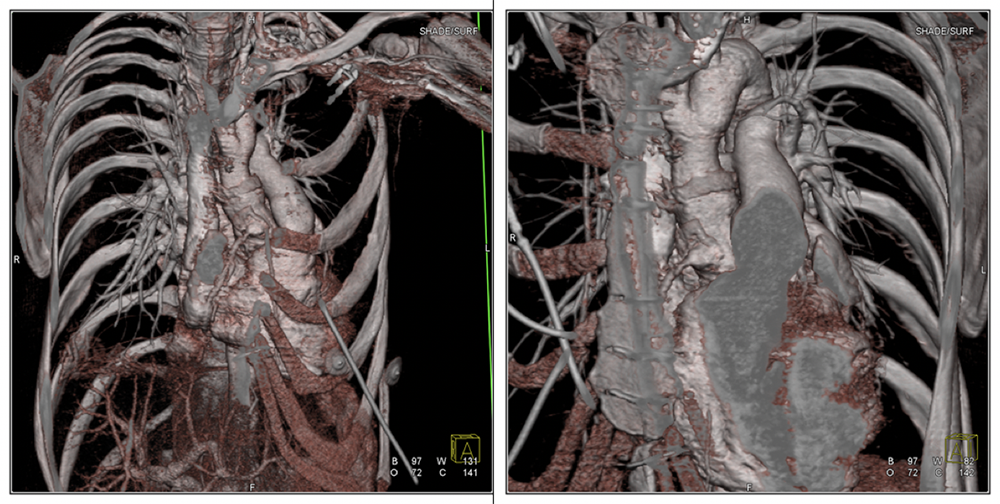 Continued… 3D color maps show contour defect related to surgical repair and vascular graft placement. See arrows. The right coronary artery re-implantation site is also well visualized. |
Case 4: Dissection following aortic root replacement 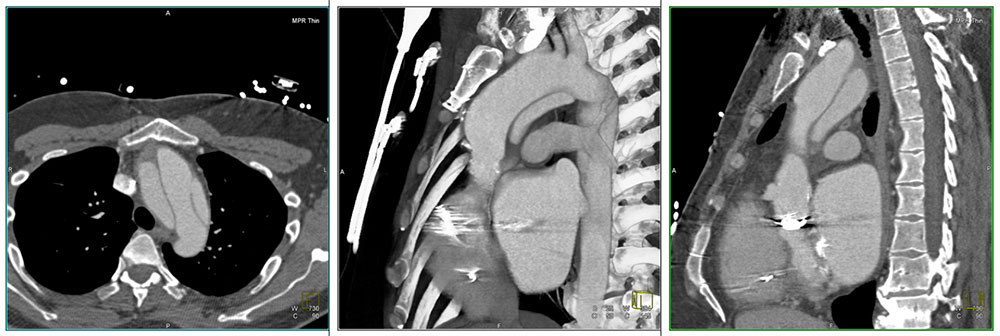 40 year old male presented with chest pain. Patient had history of aortic root replacement with composite graft. Reformatted axial and sagittal CT images demonstrated focal Type A dissection of the aortic arch - limited to the aortic arch - above the level of the composite graft which terminated at the origin of the left subclavian artery. Note artifact related to prosthetic aortic valve. |
Case 4: Dissection following aortic root replacement 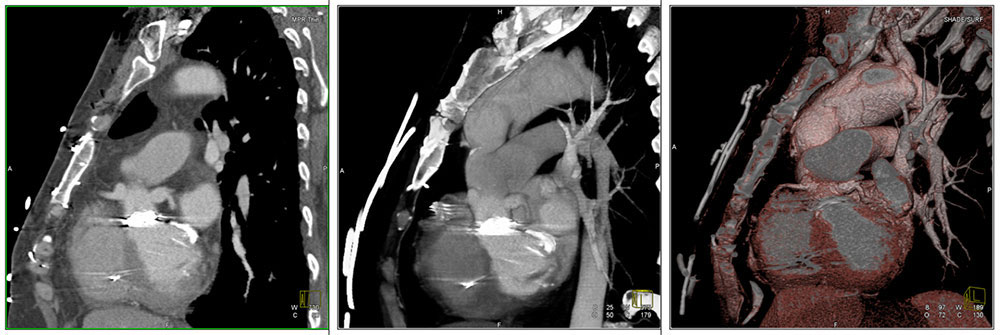 Continued… Sagittal reformatted images and sagittal 3D color map show dilatation of the origin of the coronary arteries at the site of implantation. See arrows. Again seen is artifact related to aortic and mitral valve replacement. |
Case 5: Dissection following aortic root replacement  39 year old male presented for routine follow up imaging. History of aortic root replacement with composite vascular graft. CT reformatted images as well as 3D maps show Type A dissection beginning just above the distal end of the composite graft continuing through the aortic arch and descending thoracic aorta. Note artifact related to prosthetic aortic valve. Contour defect related to graft placement best seen on the color maps. |
Case 6: Coronary artery aneurysms at site of implantation 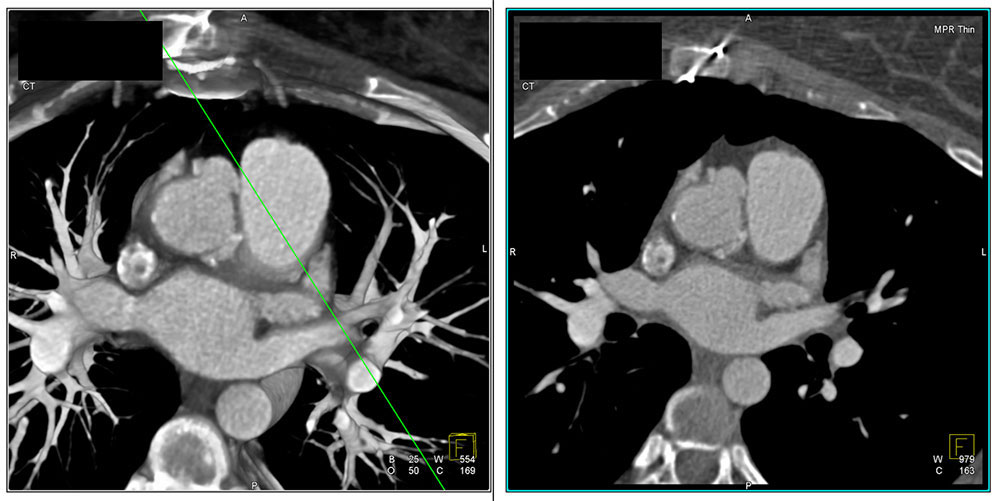 19 year old female presented for routine follow up imaging. History of aortic root replacement with composite graft. See images of normal postoperative appearance in Case 1. Axial reformatted images demonstrate dilatation of the origin of the right coronary artery just at the level of the anastomosis shown best on 3D mapping. See next slide. Also mild dilatation of the origin of the left main coronary artery. Vessel are of normal caliber distally. |
Case 6: Coronary artery aneurysms at site of implantation 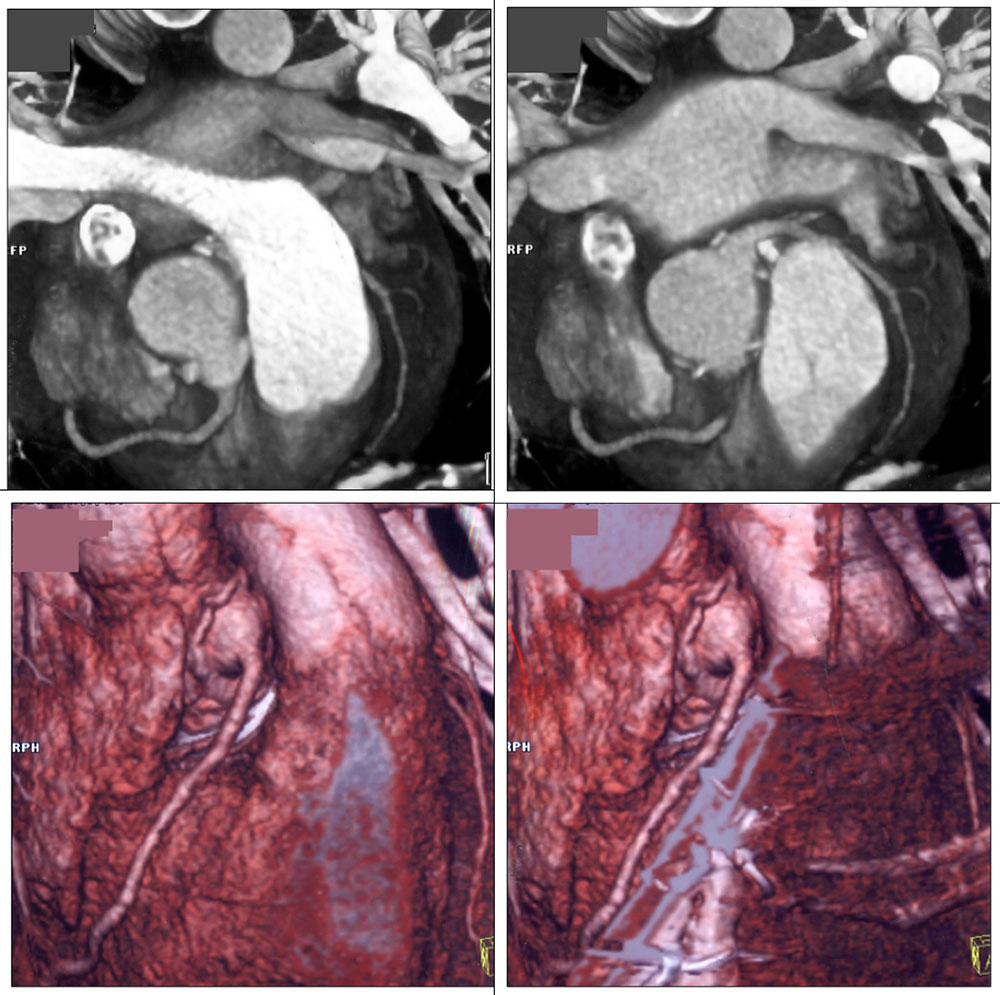 |
Case 7: Coronary artery aneurysms at site of implantation  38 year old female with history of valve-sparing aortic root replacement in 2005. On routine follow up echocardiogram found to have right coronary artery aneurysm. Reformatted images in axial and sagittal planes show focal dilatation of the origin of the right coronary artery at the anastomotic site. |
Case 7: Coronary artery aneurysms at site of implantation 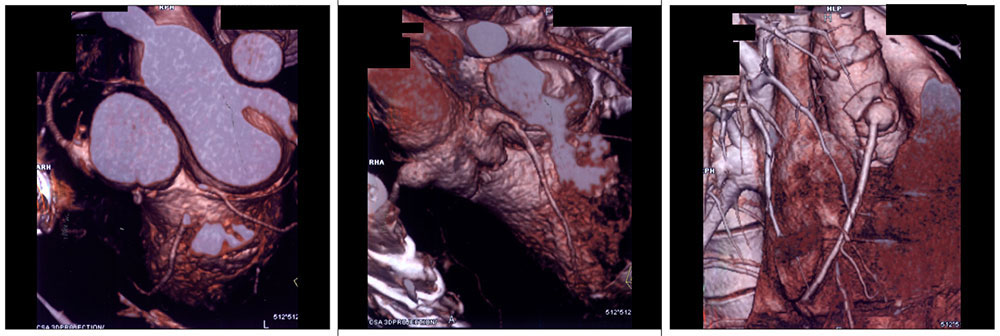 Continued… 3D color maps show focal asymmetric dilatation of the origin of the right coronary artery at the anastomotic site. Abnormality seen in all three planes. See arrows. |
Case 8: Mediastinal fluid collection 2 years after surgery 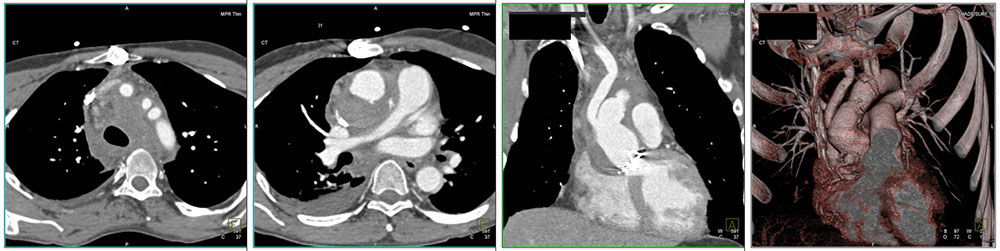 34 year old male admitted for chest pain and fever. 2 years prior to admission had aortic root replacement with composite graft. Note artifact related to aortic valve replacement. CT showed perigraft low attenuation material measuring 45-55 HU which exerts mild mass effect on right main pulmonary artery. No evidence of contrast leak or active extravasation. No pseudoaneurysm. 3D map better delineates the vascular graft and coronary artery implantation site. |
Case 9: Dilatation of the aortic sinuses and aortic root 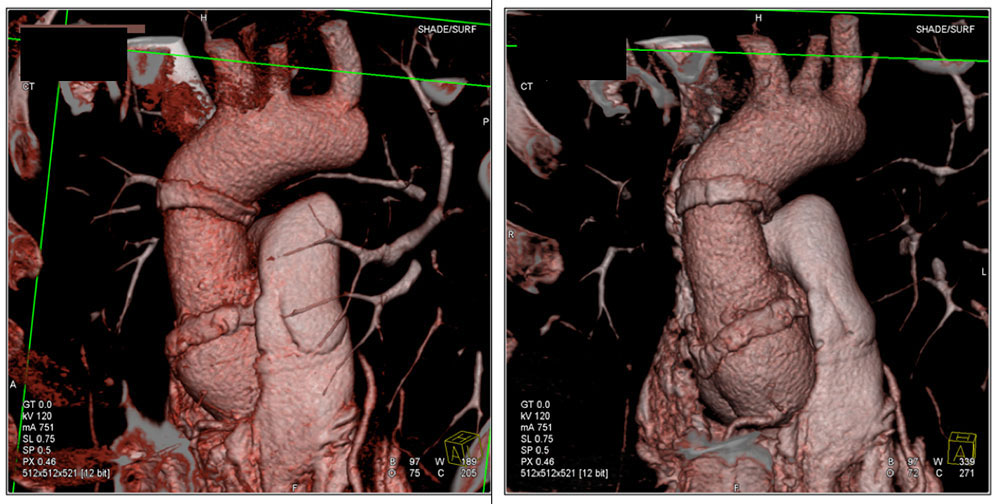 38 year old male presented with chest pain. Evidence of prior aortic root replacement with composite graft. See arrows delineating the vascular graft itself. This is best seen on the 3D color maps. |
Case 9: Dilatation of the aortic sinuses and aortic root  Continued… Reformatted images show dilatation of the aortic root below the level of the composite graft. |
Conclusion
|
References
|
References
A A Chudgar MD D Cameron MD P T Johnson MD K M Horton MD F M Corl MS E K Fishman MD |