-
Background
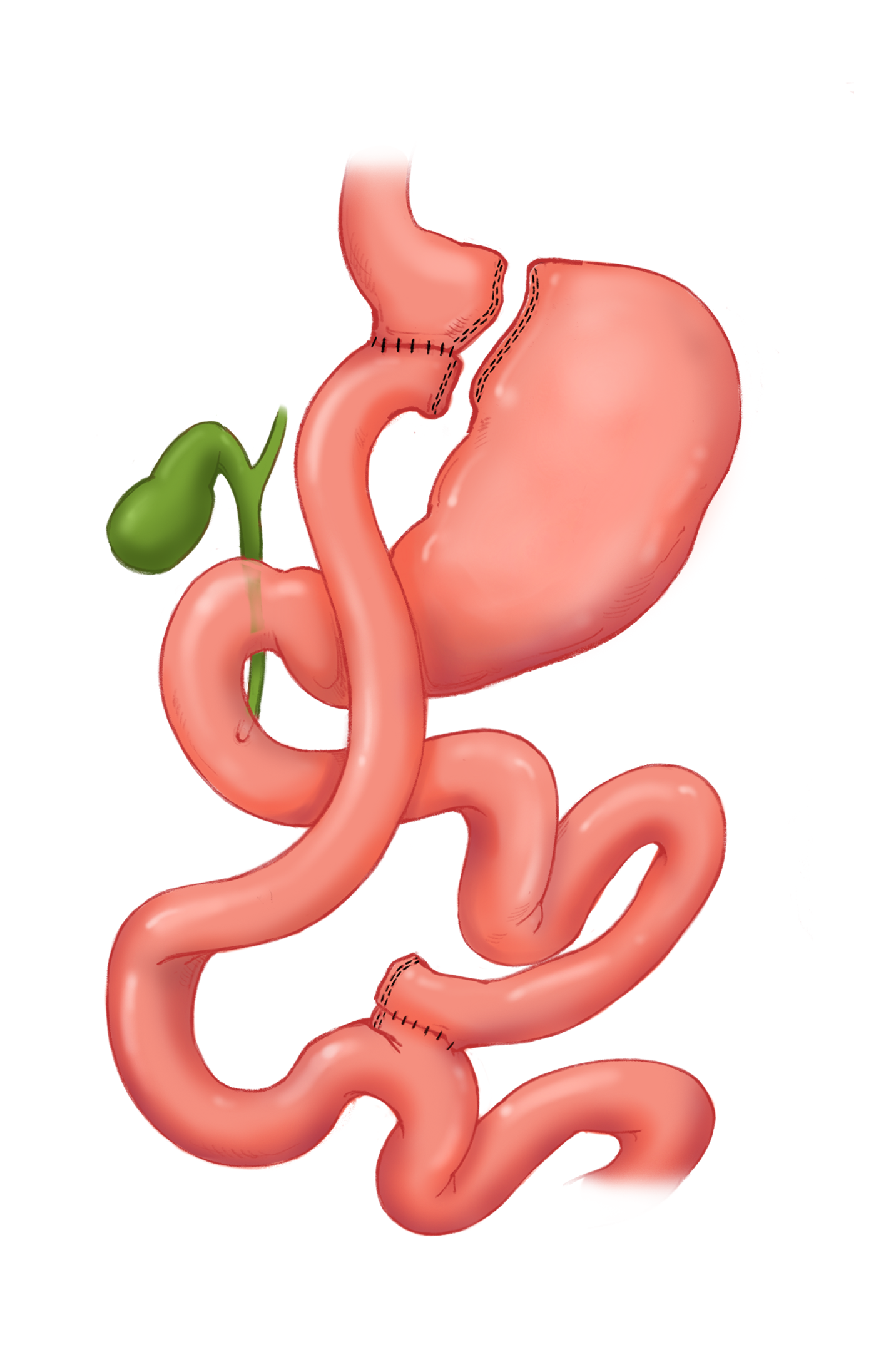
What is Roux-en-Y Gastric Bypass?
- Most common bariatric surgery, most often performed laparoscopically.
- Division of the stomach by stapling into a small pouch and attaching this pouch directly to the jejunum, Roux limb.
- Weight loss is due to restriction and malabsorption.
Indications
- Morbid obesity with BMI >40 kg/m2
- Morbid obesity with BMI 35-39.9 kg/m2 with at least one serious comorbidity such as : Type 2 Diabetes, Hypertension, Hyperlipidemia, NASH, NAFLD, OSA, ....
- Morbid obesity with BMI 30-34.9 kg/m2 AND Uncontrolled type 2 or Metabolic Syndrome
Contraindications
- Crohn's disease
- Chronic glucocorticoid or nonsteroidal anti-inflammatory use
- Uncontrolled psychiatric illness
- Coagulopathy
-
Operative Procedure
Laparoscopic
- Division of the falciform ligament
- Creation of retrocolic or antecolic passageway of the Roux limb
- Jejunojejunal (JJ) anastomosis
- Creation of gastric pouch
- Gastrojejunal (GJ) anastomosis
- Intraoperative leak test
- Closure of the potential hernia sites
- Drain placement
Considerations
- Bypass length
- Antecolic vs retrocolic passage of the Roux limb
Advantages
- Similar to sleeve gastrectomy in terms of weight loss.
- Better suited for patients with GERD or Barret's esophagus
-
Normal Post Operative Appearance
What is Roux-en-Y Gastric Bypass? CT Case Study 1 CT Case Study 2 Medical Illustration
- Most common bariatric surgery, most often performed laparoscopically.
- Division of the stomach by stapling into a small pouch and attaching this pouch directly to the jejunum, Roux limb.
- Weight loss is due to restriction and malabsorption.
-
Complications
Dumping Syndrome
- Most common complication up to 50%
- Post prandial flushing, diaphoresis, palpitations, and diarrhea.
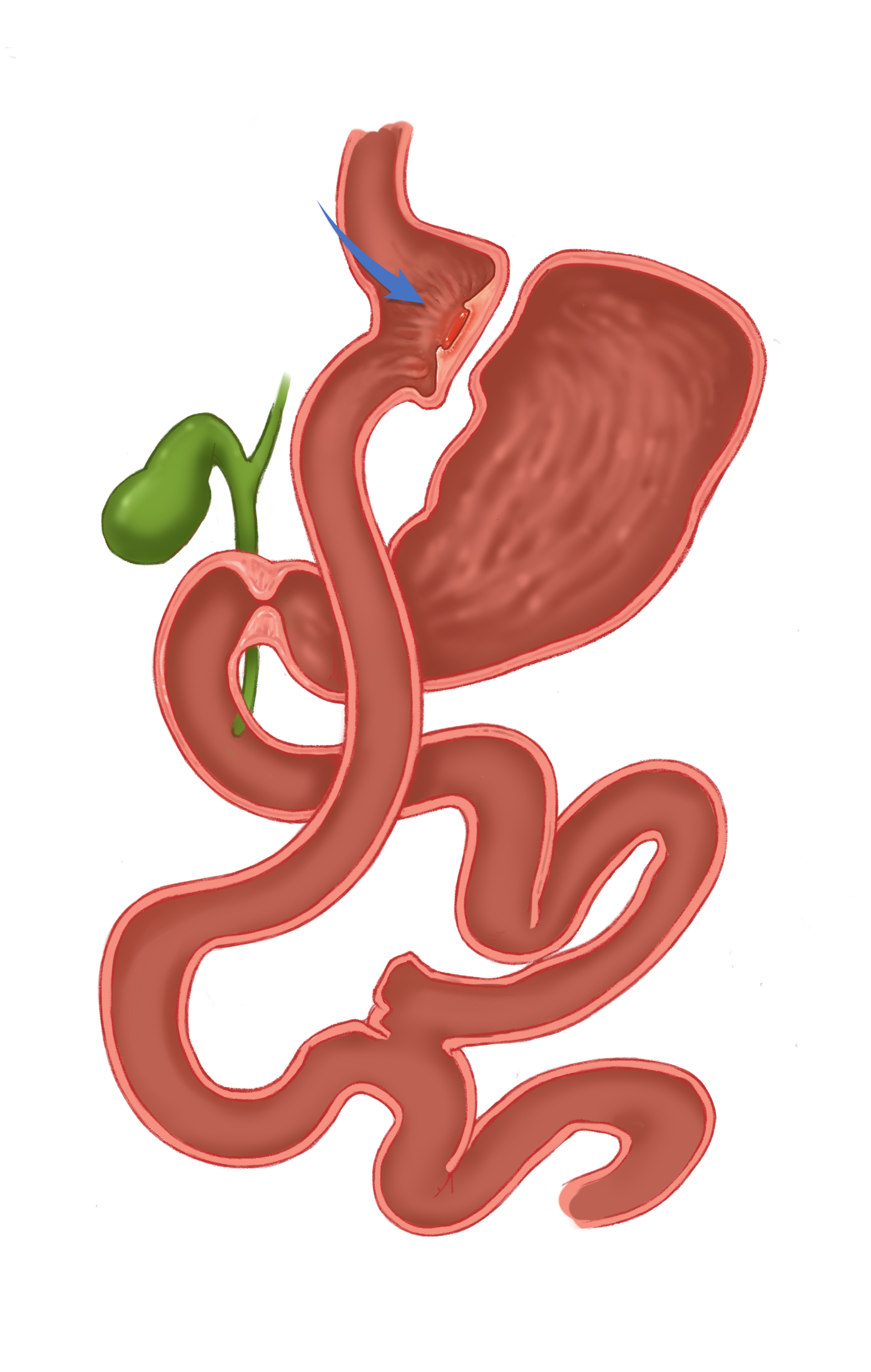
Anastomotic Stenosis
- 6-20 % develop stromal stenosis(less than 10 mm in diameter) at the anastomosis site several weeks post-op.
Marginal Ulcers CT Case Study 1 CT Case Study 2 Medical Illustration
- 1-16 % develop marginal ulcers near the gastrojejunostomy due to gastric acid injuring the jejunal mucosa.
- Other causes include gastrogastric fistula, ischemia at anastomosis, foreign material such as staples, NSAIDs use, or H-Pylori.
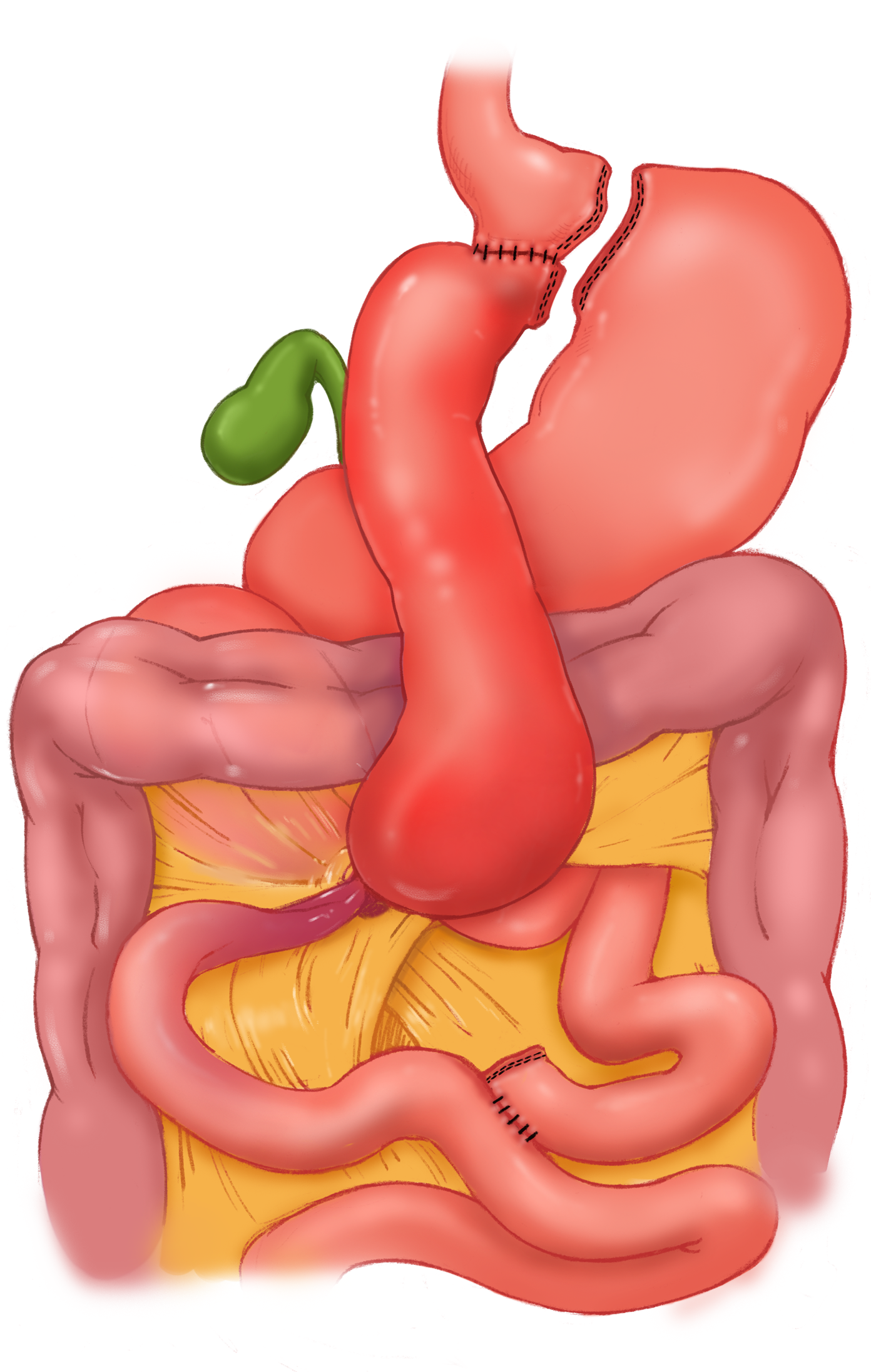
Internal Hernia Medical Illustration
- Less than 5%
Cecal Volvulus CT Case Study
- Cecal volvulus is an uncommon complication, with a few cases reported in the liturature.
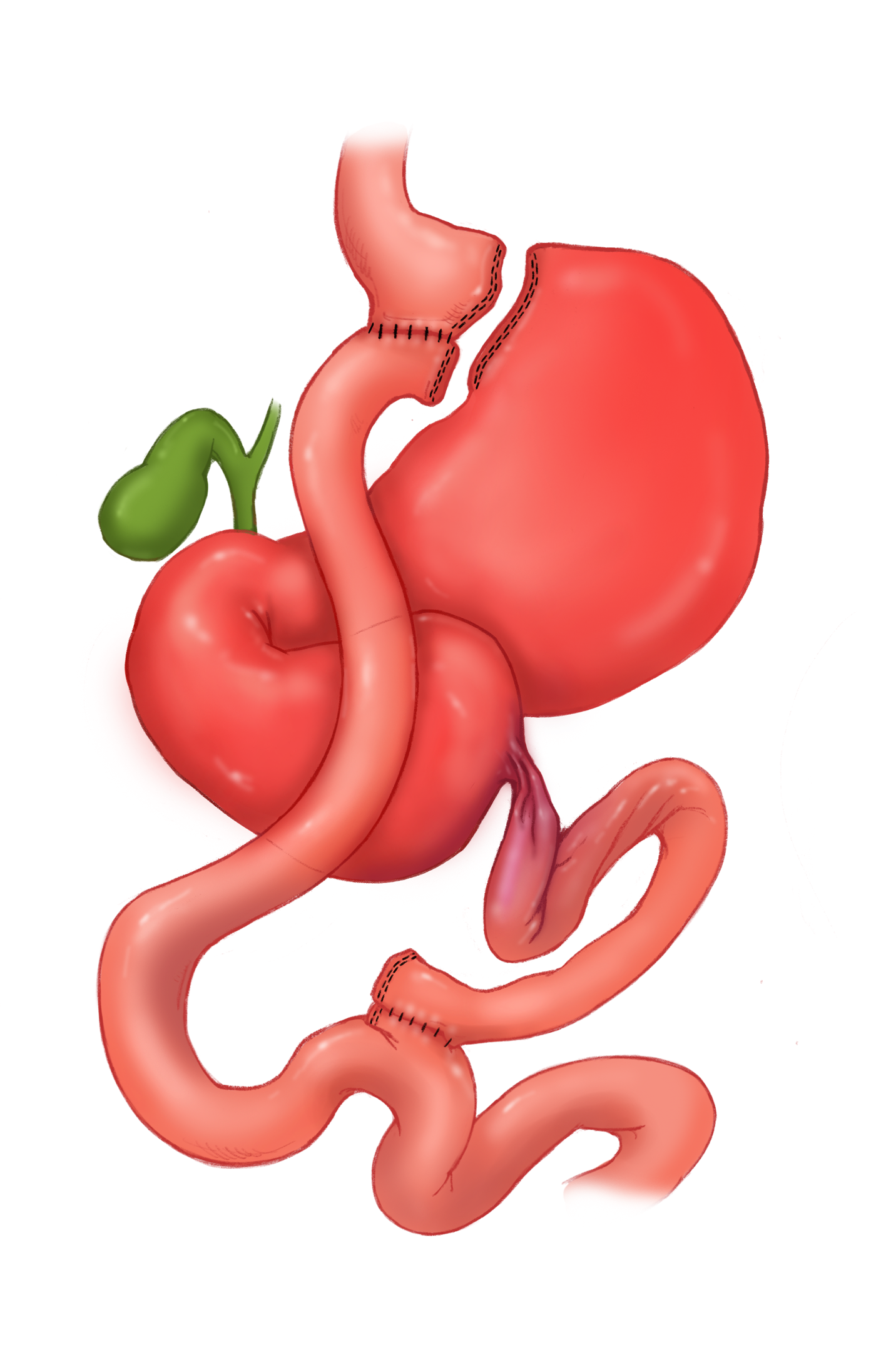
Small Bowel Obstruction CT Case Study 1 CT Case Study 2 Medical Illustration
- Less than 5%
Leak
- Less risk than gastric sleeve (2.4 versus 0.7%)
Gastrogastric fistula CT Case Study 1 CT Case Study 2 Medical Illustration
- 1-2 %
- Associated with marginal ulcer and weight regain.
Gastric remnant distention
- Rare but potentially lethal due to rupture.
Candy cane Roux syndrome
- Patients present with postprandial pain relieved by vomiting
- The afferent loop is distended with food, relieved when it empties into the Roux limb or vomited out
Other: short bowel syndrome, cholelithiasis, nephrolithiasis, incisional hernias
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
All Rights Reserved.
www.CTISUS.com