|
-- OR -- |
|
- “Non-traumatic thoracic aorta emergencies are acute conditions associated with substantial morbidity and mortality. In the emergency setting, timely detection of aortic injury through radiological imaging is crucial for prompt treatment planning and favorable patient outcomes. 3D cinematic rendering (CR), a novel rendering algorithm for computed tomography (CT) image processing, allows for life-like visualization of spatial details and contours of highly complex anatomic structures such as the thoracic aorta and its vessels, generating a photorealistic view that not just adds to diagnostic confidence, but is especially useful for non-radiologists, including surgeons and emergency medicine physicians. In this pictorial review, we demonstrate the utility of CR in the setting of non-traumatic thoracic aorta emergencies through 10 cases that were processed at a standalone 3D CR station at the time of presentation, including its role in diagnosis and management.”
Cinematic rendering of non-traumatic thoracic aorta emergencies: a new look at an old problem.
Yasrab M, Rizk RC, Chu LC, Fishman EK.
Emerg Radiol. 2024 Jan 18. doi: 10.1007/s10140-024-02204-6. Epub ahead of print. - “Routinely employed 3D post-processing tools include maximum intensity projection (MIP) and volume rendering (VR) that allow for the generation of angiographic images and a more intuitive and interactive representations of the spatial information in the dataset, respectively. Improving upon traditional VR, 3D cinematic rendering (CR) is a Food andDrug Administration (FDA)-approved technique that employs a novel lighting model to generate photorealistic images. CR involves global illumination and path tracing models whereby numerous light rays from all directions propagate through and interact with the volumetric data to generate a voxel. Complex anatomical relations are better evaluated and enhanced depth and shape perception is achieved as the technique considers a natural lighting environment and its effects (e.g., reflection, diffusion, refraction). Postprocessing windowing and the use of clip planes/masks allow cutting into the volume and isolation of the area/organ of interest.”
Cinematic rendering of non-traumatic thoracic aorta emergencies: a new look at an old problem.
Yasrab M, Rizk RC, Chu LC, Fishman EK.
Emerg Radiol. 2024 Jan 18. doi: 10.1007/s10140-024-02204-6. Epub ahead of print. - “There are some limitations that come with 3D CR. Notably, shadows generated in the images might conceal certain pathologies when viewed from specific angles, necessitating meticulous optimization and assessment from diverse angles in conjunction with the multiplanar reformations. Thus, while an initial learning period to become adept in handling and familiarizing themselves with the CR process is required for radiologists, as demonstrated in our case studies, an experienced radiologist can efficiently execute the rendering process in under 5 min.”
Cinematic rendering of non-traumatic thoracic aorta emergencies: a new look at an old problem.
Yasrab M, Rizk RC, Chu LC, Fishman EK.
Emerg Radiol. 2024 Jan 18. doi: 10.1007/s10140-024-02204-6. Epub ahead of print. - “Color mapping of different phases enhances visualization of the key pathology, such as the flow through the false and true lumens in a dissection that can be delineated by high contrast shading. CR rendering emphasizes textural changes attributable to inflammatory processes with realistic shadowing that is otherwise difficult to appreciate. The improved surface detail helps characterize an impending PAU or the nature of outpouchings suspicious for mycotic aneurysms and gives a clearer view of multiple plaques and sites of ulceration that could be otherwise missed.”
Cinematic rendering of non-traumatic thoracic aorta emergencies: a new look at an old problem.
Yasrab M, Rizk RC, Chu LC, Fishman EK.
Emerg Radiol. 2024 Jan 18. doi: 10.1007/s10140-024-02204-6. Epub ahead of print. - “Another application of 3D CR is via the black blood cinematic rendering (BBCR) preset.. BBCR is a preset we specifically developed to visualize intraluminal contours and structures of the heart and great vessels, all through adjustments that can be madein under a minute. This is especially useful in the setting of visualizing various zones of thrombi and occlusion, the degree of obstruction, and the subtle irregularities and internal arrangement of the thrombus that can only be appreciateddue to enhanced depth perception and shadowing.”
Cinematic rendering of non-traumatic thoracic aorta emergencies: a new look at an old problem.
Yasrab M, Rizk RC, Chu LC, Fishman EK.
Emerg Radiol. 2024 Jan 18. doi: 10.1007/s10140-024-02204-6. Epub ahead of print. - “The intrinsic features of 3D CR with its ability to provide a holistic field of view of the vascular map increases confidence in management and surgical planning. A global viewing angle of the thoracic aorta helps in tracking the dissection and its involvement of the aorta and the extent of mediastinal and pericardial bleeding where present .In cases where patients underwent thoracic endovascular aortic repair (TEVAR), coiling, or graft repairing, CR adds to surgical planning by improved depth perception, shadow effects, and realistic textures, demonstrating the anatomical relationships of the thoracic aorta, surrounding structures, and the pathology to be addressed, with photorealism providing the surgeon a familiar perspective to work with.”
Cinematic rendering of non-traumatic thoracic aorta emergencies: a new look at an old problem.
Yasrab M, Rizk RC, Chu LC, Fishman EK.
Emerg Radiol. 2024 Jan 18. doi: 10.1007/s10140-024-02204-6. Epub ahead of print. - “3D cinematic rendering (CR) represents an important advancement in radiological imaging, particularly in enhancing the visualization of complex anatomical structures and systems such as the thoracic aorta and its vessels. CR provides detailed, photorealistic illustrations crucial for diagnosis and surgical planning as we have seen in several cases. Future research is needed to evaluate CR’s diagnostic accuracy, both prospectively and in head-to-head comparisons with other rendering methods, as well as its role in other domains such as patient education and medical training. CR, therefore, is emerging as a promising, evolving tool for radiologists, surgeons, and the patients they treat.”
Cinematic rendering of non-traumatic thoracic aorta emergencies: a new look at an old problem.
Yasrab M, Rizk RC, Chu LC, Fishman EK.
Emerg Radiol. 2024 Jan 18. doi: 10.1007/s10140-024-02204-6. Epub ahead of print.
- "The “hard” or overt signs of extremity arterial injury include active pulsatile bleeding; rapidly expanding hematoma; palpable thrill/audible bruit; or classic signs of severe acute limb ischemia (a.k.a. 5 “P”: pulselessness, pallor, paresthesia, pain, and paralysis). The presence of these hard signs correlates with high probability of vascular injury and need of invasive management. In cases where hard signs are present and intervention is indicated, exact localization and characterization of the vascular injury is necessary (ie, multiple extremity fractures or shotgun wound), and the trauma team may pursue CTA imaging if the clinical condition permits and the study can be obtained in a timely fashion.”
Computer Tomography Angiography of Peripheral Vascular Injuries
Fabio M. Paes, MD, Felipe Munera
Radiol Clin N Am 61 (2023) 141–150 - “The “soft” signs of extremity arterial injury include history of arterial bleeding at the scene of trauma or in transit; proximity of a penetrating wound or blunt injury to an artery; small nonpulsatile hematoma over an artery; and neurologic deficit originating in a nerve adjacent to a named artery. The incidence of arterial injuries in such trauma patients ranges from 3% to 25%, depending on which individual soft sign or combination of signs is present. In patients presenting with soft signs and ankle brachial index (ABI) or arterial pressure index (API) less than 0.9, further imaging (CTA or duplex ultrasound) is usually indicated.”
Computer Tomography Angiography of Peripheral Vascular Injuries
Fabio M. Paes, MD, Felipe Munera
Radiol Clin N Am 61 (2023) 141–150 - “The continuous advances of CT technology have improved image quality, permitted faster acquisition and imaging reconstruction times, and allowed incorporation of postprocessing techniques to routine readings with the use of curved multiplanar reformats, maximum intensity projection (MIP), bone subtraction, trajectography, and three dimensional (3D) volume-rendering.”
Computer Tomography Angiography of Peripheral Vascular Injuries
Fabio M. Paes, MD, Felipe Munera
Radiol Clin N Am 61 (2023) 141–150 - “At our institution, the submillimeter isotropic voxel data set is routinely reconstructed at 1.5 and 3.0 mm in the conventional axial plane and submitted for evaluation. Multiplanar reconstructions on sagittal and coronal planes along the axis of the extremity as well as MIP images are also obtained by technologists at the scanner. 3D volume rendering images and curved planar reformats, including trajectography, can be requested or constructed using postprocessing software available on the workstations.”
Computer Tomography Angiography of Peripheral Vascular Injuries
Fabio M. Paes, MD, Felipe Munera
Radiol Clin N Am 61 (2023) 141–150 - “There are 5 recognized types of acute vascular injuries with corresponding imaging findings.: (1) intimal tears (intimal flaps, surface disruptions, or subintimal/intramural hematomas), (2) full thickness vessel wall defects with pseudoaneurysms or hemorrhage, (3) complete transections with active hemorrhage and/or occlusion, (4) arteriovenous fistulas (AVF), and (5) spasm. Low-grade intimal injuries and/or intramural hematomas are more often associated with blunt trauma and can lead to secondary occlusion. Full thick wall defects, complete transections, and AVF usually occur with penetrating trauma. Spasm is a temporary finding more common in young patients, which can occur after blunt or penetrating trauma.”
Computer Tomography Angiography of Peripheral Vascular Injuries
Fabio M. Paes, MD, Felipe Munera
Radiol Clin N Am 61 (2023) 141–150 - “Arterial transections occur when the circumference of the vessel is disrupted and usually leads to active contrast extravasation from the proximal segment and/or thrombotic occlusion of the disconnected distal artery. As for traumatic venous injuries in the extremity, wall defects in many peripheral veins seem to heal when local tissue pressure is applied which prevents significant extravasation of blood in most traumatic cases.”
Computer Tomography Angiography of Peripheral Vascular Injuries
Fabio M. Paes, MD, Felipe Munera
Radiol Clin N Am 61 (2023) 141–150 - “Metallic projectiles retained in soft tissues, bone fragments, and orthopedic hardware can result in significant artifacts, commonly limiting the evaluation of adjacent vessels, and obscuring or creating“false” vascular injury imaging findings. Often, adequate contrast opacification of the vessels and the use of multiplanar reformats still alloevaluation of large vessels and the diagnosis of major traumatic injuries. In cases where the streak artifact precludes the evaluation of the vascular bed in question, DSA may be indicated to evaluate and exclude the presence of vascular injury. Recent imaging advancements using metal artifact reduction algorithms and/or DECT have shown to decrease metal and/or bone fragment artifacts, improving visualization of the of the soft-tissues and bones details, and as such can be useful to evaluate vascular injuries.”
Computer Tomography Angiography of Peripheral Vascular Injuries
Fabio M. Paes, MD, Felipe Munera
Radiol Clin N Am 61 (2023) 141–150 - • Peripheral vascular injuries account for 40% to 75% of all vascular injuries treated in civilian trauma centers.
• Extremity vascular injury is more often associated with penetrating trauma (75% to 80% of cases in urban trauma centers) than blunt trauma (5%–25% of cases), and among the penetrating mechanisms, more often after a gunshot wound than a stab wound.
• CTA is a highly effective tool for the detection and characterization of peripheral vascular injuries with proven outstanding sensitivities in the range of 95% to 100%, specificities of 87% to 100%, and accuracy around 93%.
Computer Tomography Angiography of Peripheral Vascular Injuries
Fabio M. Paes, MD, Felipe Munera
Radiol Clin N Am 61 (2023) 141–150 - • Patient preparation is key to obtain optimal diagnostic images of the peripheral vessels. Adequate IV access, iodine contrast flow, patient position, and lack of motion are all important to avoid the formation of imaging artifacts and allow adequate imaging evaluation.
• AVF is differentiated from asymmetric hyperemia and early venous return on the injured extremity by having the contrast density in the opacified venous segment of the fistula approaching the adjacent artery.
Computer Tomography Angiography of Peripheral Vascular Injuries
Fabio M. Paes, MD, Felipe Munera
Radiol Clin N Am 61 (2023) 141–150
- "Rapid deceleration is the universal mechanism of this injury. Most commonly, there are multiple other life- threatening injuries present with less than 20% having this as an isolated injury making the diagnosis and initial next steps challenging. BTAI is defined as a tear in the aorta that is a result of a combination of shear and stretch forces, rapid deceleration, increased intravascular pressure and compression of the aorta between the anterior chest wall and vertebrae.”
Blunt thoracic aortic injury – concepts and management
Nicolas J. Mouawad et al.
Journal of Cardiothoracic Surgery (2020) 15:62 - “Up to 80% of patients presenting with blunt thoracic aortic injury(BTAI) die before hospitalization, and in the remaining survivors, in- hospital mortality is as high as 46%. While this is a potentially lethal injury, it is rare and accounts for 1.5% of thoracic trauma.”
Blunt thoracic aortic injury – concepts and management
Nicolas J. Mouawad et al.
Journal of Cardiothoracic Surgery (2020) 15:62 - "Injury can occur along the entire length of the aorta, essentially from the ascending aorta to the iliac bifurcation, although the injury typically occurs areas of aortic tethering, notably the aortic isthmus.”
Blunt thoracic aortic injury – concepts and management
Nicolas J. Mouawad et al.
Journal of Cardiothoracic Surgery (2020) 15:62 - “Blunt thoracic aortic trauma is associated with other major entities of chest trauma, including, but not limited to, sternal fracture, 1st/2nd rib fractures, clavicle and/or scapular fractures, pneumothoraces, hemothoraces, flail chest, pulmonary contusions, diaphragm injury, tracheobronchial disruption and esophageal injuries; these should raise suspicion for BTAI.”
Blunt thoracic aortic injury – concepts and management
Nicolas J. Mouawad et al.
Journal of Cardiothoracic Surgery (2020) 15:62 - "Injuries are assigned one of 4 grades based on CTA imaging: grade 1 (intimal tear), grade II (intramural hematoma), grade III (pseudoaneurysm) and grade IV (rupture). Currently, the recommendation is to proceed with surgical repair of Grade II-IV injuries [20]. For grade I injuries, it is well established that no intervention is necessary as these tend to resolve on their own with conservative management. Grade II injures do fall into a “gray zone” between medical management and operative intervention although more recent studies do document that nonoperative is safe with close follow up.”
Blunt thoracic aortic injury – concepts and management
Nicolas J. Mouawad et al.
Journal of Cardiothoracic Surgery (2020) 15:62 - "Blunt thoracic aortic injury requires a high index of suspicion based on mechanism of injury in the trauma population. Endovascular approaches have slowly replaced open surgical repair for the management of this pathology. Clearly, such patients that present with blunt thoracic injury should be relegated to centers that specialize in the polytrauma patient as it is their concurrent injuries that are the focus of their critical care.”
Blunt thoracic aortic injury – concepts and management
Nicolas J. Mouawad et al.
Journal of Cardiothoracic Surgery (2020) 15:62 - “The CT findings of TAI can be divided into direct signs of injury and indirect or associated findings. Direct findings of aortic injury include intramural hematoma, intimal flap and pseudoaneurysm. Injuries that only involve the intima, classified as minimal aortic injuries, should only have direct findings of TAI. Minimal aortic injuries can present with an intimal flap, intraluminal aortic thrombus or intramural hematoma. With the improvement in technology allowing thinner CT slice thickness minimal aortic injuries are being diagnosed more frequently.”
Traumatic aortic injury: CT findings, mimics, and therapeutic options
Ethany L. Cullen et al.
Cardiovasc Diagn Ther 2014;4(3):238-244 - "Ductal remnants, a diverticulum or small bump, are normal remnants of the embryologic ductus arteriosus. This normal variant can simulate injury and can be very perplexing for the inexperienced or unaware radiologist. The ductal diverticulum is a remnant of the closed or partially closed ductus arteriosus which connects the pulmonary artery to the aorta in fetal circulation. Ductal remnants are located at the inferior surface of the aortic arch near the aortic isthmus which leads to their confusion with TAIs. Ductal remnants are typically smooth walled and have obtuse margins that are continuous with the aortic wall and are often calcified. The presence of calcification can be very helpful in distinguishing a ductal remnant from a TAI with the presence of calcification favoring a benign ductal remnant.”
Traumatic aortic injury: CT findings, mimics, and therapeutic options
Ethany L. Cullen et al.
Cardiovasc Diagn Ther 2014;4(3):238-244 - "Mediastinal hematomas can be due to injury to other structures including the pulmonary artery, great vessels or mediastinal veins, or even fractures of vertebral bodies. Presence of a mediastinal hematoma should prompt a careful search for an aortic, pulmonary artery or great vessel injury. In the absence of an identified arterial injury the hematoma is likely venous. A preserved fat plane around the aorta or hematoma centered away from the aorta is less likely to be associated with aortic injury and more likely to be venous.”
Traumatic aortic injury: CT findings, mimics, and therapeutic options
Ethany L. Cullen et al.
Cardiovasc Diagn Ther 2014;4(3):238-244 - "The best way to distinguish a true aortic root injury from motion artifact is to repeat thoracic imaging with ECG gating; and echocardiography can be a reasonable alternative. The difference between a study done without and with ECG gating is illustrated in. In our institution all of the chest CT done as part of a trauma survey are acquired without ECG gating. Since the majority of TAIs are at the aortic isthmus, which is typically well seen on non-gated studies, we feel the additional radiation exposure and time required for setup and acquisition of an ECG gated study is not necessary for every patient.”
Traumatic aortic injury: CT findings, mimics, and therapeutic options
Ethany L. Cullen et al.
Cardiovasc Diagn Ther 2014;4(3):238-244 - “Blunt aortic injuries (BAI) represent the second leading cause of death from motor vehicle crashes accounting for 15% of all motor vehicle accident-associated deaths. Death occurs at the scene of the accident in 70–90% of the cases. According to historical case series, the majority of the patients with BAI (75%) who arrive to the hospi- tal alive are hemodynamically stable, but only 10% survive more than 6 h. Patients arriving to the hospital alive most frequently present with injury at the aortic isthmus where periadventitial tissue seems to provide some degree of protection against free rupture. The majority of patients with BAI have an associated closed head injury, multiple rib fractures, lung contusions, or orthopedic injuries.”
Blunt aortic injuries in the new era: radiologic findings and polytrauma risk assessment dictates management strategy
Rachel Elizabeth Payne et al.
European Journal of Trauma and Emergency Surgery (2019) 45:951–957 - “The SVS AI grading system is based on the following criteria: (grade I) intimal tear; (grade II) intramural hematoma; (grade III) pseudoaneurysm; (grade IV) rupture. Under this system, grade I-II are considered mild and grade III-IV are considered severe. In our investigation, we created criteria for radiographic severe injury and used this as a binary variable (severe versus the others) rather than creating a full grading system.”
Blunt aortic injuries in the new era: radiologic findings and polytrauma risk assessment dictates management strategy
Rachel Elizabeth Payne et al.
European Journal of Trauma and Emergency Surgery (2019) 45:951–957 - “Radiographically severe injuries were those meeting any of the following criteria: total/partial aortic transection, active contrast extravasation, or the association of 2 of more of the following: contained contrast extravasation > 10 mm, periaortic hematoma and/or mediastinal hematoma thicker than 10 mm, or significant left pleural effusion. We evaluated multiple inju- ries where a pseudoaneurysm was found in isolation, without significant associated hematoma or extravasation, which did not meet criteria for RSI. Thus, many injuries that would be graded III by the SVS system were not included in our RSI classification since they did not meet our selection criteria.”
Blunt aortic injuries in the new era: radiologic findings and polytrauma risk assessment dictates management strategy
Rachel Elizabeth Payne et al.
European Journal of Trauma and Emergency Surgery (2019) 45:951–957 - “Acute aortic injuries are not common in the setting of severe blunt trauma, but lead to significant morbidity and mortality. High- quality MDCT with 2D MPRs and 3D rendering are essential to identify aortic trauma and distinguish anatomic variants and other forms of aortic pathology from an acute injury. Misinterpretation of mimics of acute aortic injury can lead to unnecessary arteriography and thoracic surgery. Since most traumatic injuries occur in the distal arch, radiologists must be cognizant of the range of appearances of variants related to the ductus diverticulum. Cinematic rendering (CR) is a new 3D post-processing tool that provides even greater anatomic detail than traditional volume rendering. In this case series, CR is used to impart to radiologists a better understanding of various anatomic configurations that can be seen with a ductus diverticulum.”
MDCT of ductus diverticulum: 3D cinematic rendering to enhance understanding of anatomic configuration and avoid misinterpretation as traumatic aortic injury
Steven P. Rowe & Pamela T. Johnson & Elliot K. Fishman
Emergency Radiology (2018) 25:209–213 - "Among these is the ductus diverticulum—a remnant of the ductus arteriosus that arises from the lesser curvature of the aortic arch, which can be mistaken for a traumatic aortic pseudoaneurysm, dissection, or incomplete rupture. The distal aortic arch, and in particular the undersurface, is the most common location for acute traumatic aortic injury. Differentiation of a ductus diverticulum from an aortic injury can be difficult, but it is of paramount importance in order to spare patients the morbidity of unnecessary thoracic surgery. This becomes more challenging in the setting of other thoracic traumatic injury, especially mediastinal hematoma, as demonstrated in this case report.”
MDCT of ductus diverticulum: 3D cinematic rendering to enhance understanding of anatomic configuration and avoid misinterpretation as traumatic aortic injury
Steven P. Rowe & Pamela T. Johnson & Elliot K. Fishman
Emergency Radiology (2018) 25:209–213 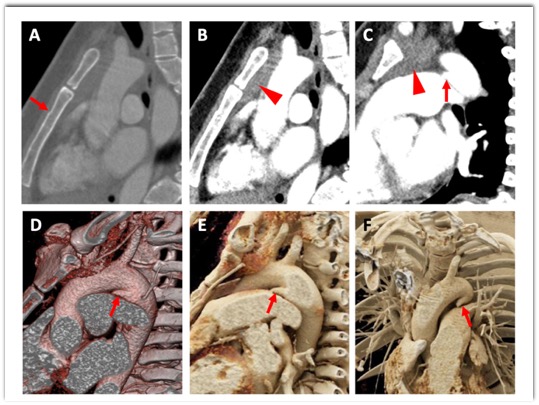
MDCT of ductus diverticulum: 3D cinematic rendering to enhance understanding of anatomic configuration and avoid misinterpretation as traumatic aortic injury
Steven P. Rowe & Pamela T. Johnson & Elliot K. Fishman
Emergency Radiology (2018) 25:209–213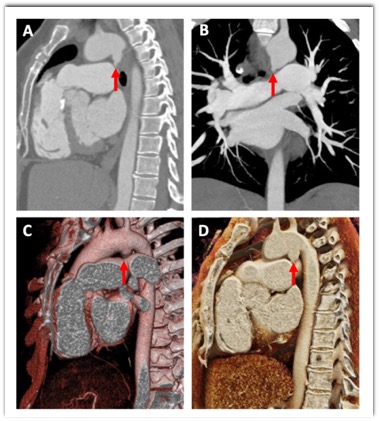
MDCT of ductus diverticulum: 3D cinematic rendering to enhance understanding of anatomic configuration and avoid misinterpretation as traumatic aortic injury
Steven P. Rowe & Pamela T. Johnson & Elliot K. Fishman
Emergency Radiology (2018) 25:209–213
- "Analyses of trauma patients who underwent upper or lower extremity CTA showed sensitivities in the range of 95–100%, specificities of 87–100%, a low nondiagnostic imaging rate, and good inter-observer agreement between radiologists indicating that CTA can replace conventional diagnostic angiography in the acute trauma setting. Several of these studies are limited by verification and follow-up bias, and although some injuries may have been missed by CTA, none of the missed injuries was likely to have been clinically significant”
Imaging primer for CT angiography in peripheral vascular trauma
Lara Walkoff et al.
Emergency Radiology (2021) 28:143–152 - "When unilateral upper extremity CTA is to be performed, an IV should be placed contralateral to the affected extremity to prevent dense venous contrast from obscuring the adjacent arteries. Optimal positioning is with the body supine with the arm over the head, palm facing upward with fingers extended. If more comfortable for the patient, prone body position- ing with the palm facing the table is also acceptable. Positioning the arm above the head helps to reduce noise; however, this may not be possible in the setting of an upper extremity injury. In such cases, the arms can be positioned at the patient’s side with images acquired in the same field-of- view as the chest, abdomen, and pelvis CT.”
Imaging primer for CT angiography in peripheral vascular trauma
Lara Walkoff et al.
Emergency Radiology (2021) 28:143–152 - "Multiplanar reconstructions in the coronal and sagittal planes are performed at the scanner. Curved planar reconstructions (CPR) and maximum intensity projection (MIP) images can be constructed at the workstation. 3D renderings produced at the workstation or in a dedicated 3D lab are offered upon ordering provider request. Vascular structures are usually best viewed with window width setting around 600 and window level setting around 80.”
Imaging primer for CT angiography in peripheral vascular trauma
Lara Walkoff et al.
Emergency Radiology (2021) 28:143–152 - “A pseudoaneurysm is an injury to the artery contained by fibrous tissue or adventitia, which is in contrast to true aneurysms which contain all three layers of the vessel wall. On CTA, a pseudoaneurysm will appear as a focal contrast-filled outpouching .In contrast to active hemorrhage, pseudoaneurysms maintain their shape on delayed phase imaging, whereas contrast will increase and change shape in the setting of active hemorrhage. Occasionally, the outpouching will not entirely fill with contrast owing to the presence of thrombus. Sometimes pseudoaneurysm can have delayed presentation with atypical clinical symptoms such as compressive neuropathy or pulsatile soft tissue mass.”
Imaging primer for CT angiography in peripheral vascular trauma
Lara Walkoff et al.
Emergency Radiology (2021) 28:143–152 - "An AVF occurs when traumatic injury results in a direct communication between an artery and an adjacent vein without an intervening capillary bed. The exact site of communication may not be visible; however, early filling of a vein adjacent to an artery in the region of traumatic injury (in the absence of venous filling in the more distal extremity) is indicative of an AVF.”
Imaging primer for CT angiography in peripheral vascular trauma
Lara Walkoff et al.
Emergency Radiology (2021) 28:143–152 - “Arterial vasospasm occurring in the setting of traumatic injury can be difficult to differentiate from dissection with a thrombosed false lumen. The etiology of vasospasm in the absence of visible endothelial injury is not entirely clear, but has been hypothesized to be related to mechanical stimulus from pressure waves transmitted from a high velocity pene- trating object and/or release of vasoconstrictive substances. Like other types of arterial injury, vasospasm is usually present adjacent to soft tissue injury or vessel segments along the path of the penetrating injury and appears as a narrowed segment of the artery. Management depends on the severity and length of the narrowed segment, but may include conventional angiography, MR angiography, or clinical monitoring with follow-up imaging to ensure resolution and differentiate from a true arterial injury.”
Imaging primer for CT angiography in peripheral vascular trauma
Lara Walkoff et al.
Emergency Radiology (2021) 28:143–152 - "Variant vascular anatomy can be a potential source of false positives results. If an artery does not arise at its conventional location, it may be mistaken for an occlusion. In a study of conventional arteriograms of the upper extremity, variants were noted in 9% of individuals, the most common being a high origin of the radial artery from the brachial artery, with high origins of the radial and ulnar artery from the axillary artery occurring less frequently. In the lower extremity, approximately 9% of individuals have variant popliteal and tibial artery branching patterns, with high origins of the anterior tibial artery being most common. In addition, the tibial arteries may be congenitally absent or hypoplastic, and in these cases should not be confused with occlusion. Findings that suggest a congenitally absent or hypoplastic tibial artery include robust remaining tibial arteries supplying the extremity in the region of the absent artery, finding present on a prior imaging study, lack of abrupt vessel cutoff, and extended distance from region of trauma.”
Imaging primer for CT angiography in peripheral vascular trauma
Lara Walkoff et al.
Emergency Radiology (2021) 28:143–152 - "Variant vascular anatomy can be a potential source of false positives results. If an artery does not arise at its conventional location, it may be mistaken for an occlusion. In a study of conventional arteriograms of the upper extremity, variants were noted in 9% of individuals, the most common being a high origin of the radial artery from the brachial artery, with high origins of the radial and ulnar artery from the axillary artery occurring less frequently. In the lower extremity, approximately 9% of individuals have variant popliteal and tibial artery branching patterns, with high origins of the anterior tibial artery being most common. In addition, the tibial arteries may be congenitally absent or hypoplastic, and in these cases should not be confused with occlusion..”
Imaging primer for CT angiography in peripheral vascular trauma
Lara Walkoff et al.
Emergency Radiology (2021) 28:143–152
- “The superficial femoral artery becomes the popliteal artery as it traverses the adductor hiatus, an opening along the insertion of the adductor magnus muscle, marking the transition from the anterior compartment of the thigh to the popliteal fossa. The vast majority (89–92%) of patients have a classical branching pattern with the popliteal artery bifurcating into an anterior tibial artery and the tibioperoneal trunk. The tibioperoneal trunk divides into the posterior tibial artery and peroneal artery (aka fibular artery), both in the posterior compartment of the leg. Other branching patterns include a two vessel runoff with hypoplastic/aplastic posterior tibial artery (3.5%) and trifurcation of the popliteal artery in the popliteal fossa (2.5%). There are at least ten different branching patterns described, with the rest occurring far less frequently.”
Computed Tomography Angiography of the Extremities in Emergencies Madhuripan N et al. Seminars in Ultrasound, CT and MRI (in press) - Blunt trauma can be secondary to motor
vehicle accidents, falls, athletic injuries and can be associated with fractures of adjacent bones. Penetrating trauma may be secondary to ballistic injury, stab injury, and may or may not be associated with bony injuries. The findings that need to be specifically sought in cases of trauma are as follows.
• Active arterial bleeding •Occlusion/transection
• Pseudoaneurysm, traumatic arteriovenous fistula
• Dissection
• Focal narrowing/spasm
Computed Tomography Angiography of the Extremities in Emergencies Madhuripan N et al. Seminars in Ultrasound, CT and MRI (in press)
- Arterial Trauma: CT Findings
• active extravasation
• subcutaneous or intra- muscular hematoma
• pseudoaneurysm
• vessel narrowing/stretching
• occlusion
• arteriovenous fistula - “Examples of anatomic landmarks include the lateral margin of the first rib that demarcates the boundary between the subclavian artery and the axillary artery, and the inferior margin of the tendons of the latissimus dorsi and teres major muscles that delineate the transition between the axillary artery and brachial artery. The normal location of the branch point of the brachial artery into the radial and ulnar arteries is at the level of the antecubital fossa near the coronoid process of the ulna. Conventional branching anatomy is seen in approximately 70% of individuals.”
Computed Tomography Angiography of the Upper Extremities Dave RB, Fleischmann D. Radiol Clin North Am. 2016 Jan;54(1):101-14 - “Examples of anatomic landmarks include the lateral margin of the first rib that demarcates the boundary between the subclavian artery and the axillary artery, and the inferior margin of the tendons of the latissimus dorsi and teres major muscles that delineate the transition between the axillary artery and brachial artery. The normal location of the branch point of the brachial artery into the radial and ulnar arteries is at the level of the antecubital fossa near the coronoid process of the ulna. Conventional branching anatomy is seen in approximately 70% of individuals.”
Computed Tomography Angiography of the Upper Extremities Dave RB, Fleischmann D. Radiol Clin North Am. 2016 Jan;54(1):101-14 - “The utility of CTA in the setting of trauma has been recognized. However, it’s less well-known and varied clinical applications in the subacute setting are also important and include presurgical anatomic mapping including identification of variant arterial anatomy, evaluation of connective disorders, vasculitis, overuse syndromes, AV fistula/grafts, vascular malformations, compression syndromes, and assessment of perivascular pathology. Volume-
rendered, maximum intensity projection, and mul- tiplanar reformat images are indispensable for evaluating the data set.”
Computed Tomography Angiography of the Upper Extremities Dave RB, Fleischmann D. Radiol Clin North Am. 2016 Jan;54(1):101-14
- “Indication for total body computed tomography (CT) is based on the presence of signs and symptoms of vascular damage at clinical examination. Patients are immediately transferred in the operating room for surgery if more serious injuries that require immediate surgical care are not diagnosed, or hemostasis may be preliminary reached in the emergency room. Hemodynamically stable patients with no history and clinical examination showing suspected vascular damage are allowed in the radiology department for obtaining a total body CT scan with intravenous contrast medium and then transferred to the surgical ward trauma for observation.”
Imaging assessment of gunshot wounds. Reginelli A et al. Semin Ultrasound CT MR. 2015 Feb;36(1):57-67. - “Multi-detector computed tomography angiography (MDCTA) of the lower extremities is an integral part of the decision-making process of lower extremity trauma. MDCTA can be integrated into multiphasic whole-body trauma MDCT and has replaced the traditional gold standard of catheter-based angiography as the preferred technique for the initial assessment of lower extremity trauma in many institutions worldwide. Advances in MDCT technology enable high speed simultaneous evaluation of both complete lower extremities, rapid image reconstruction, and advanced image visualization for the noninvasive and accurate diagnosis of vascular, including hematoma, active extravasation, vasospasm, stenosis, external compression, occlusion, intimal injury and dissection, arteriovenous fistulas, and pseudoaneurysm formation.”
State-of-the-art 3DCT angiography assessment of lower extremity trauma: typical findings, pearls, and pitfalls. Fritz J, Efron DT, Fishman EK. Emerg Radiol. 2013 Jun;20(3):175-84 - “Advances in MDCT technology enable high speed simultaneous evaluation of both complete lower extremities, rapid image reconstruction, and advanced image visualization for the noninvasive and accurate diagnosis of vascular, including hematoma, active extravasation, vasospasm, stenosis, external compression, occlusion, intimal injury and dissection, arteriovenous fistulas, and pseudoaneurysm formation.”
State-of-the-art 3DCT angiography assessment of lower extremity trauma: typical findings, pearls, and pitfalls. Fritz J, Efron DT, Fishman EK. Emerg Radiol. 2013 Jun;20(3):175-84 - “The subclavian artery continues as the axillary artery after crossing the lateral margin of the first rib. Its major branches include the superior thoracic, thoracoacromial, lateral thoracic, subscapular, and anterior and posterior humer- al circumflex arteries. These branches supply muscles of the shoulder girdle, humerus, scap- ula, and chest wall. After coursing beyond the inferior lateral margin of the teres major mus- cle, the axillary artery becomes the brachial artery.” CT Angiography of the Upper Extremity Arterial System: Part 1—Anatomy, Technique, and Use in Trauma Patients Bozlar U et al. AJR 2013; 201:745–752
- “The brachial artery courses along the medial aspect of the upper arm and gives rise to the deep brachial artery and smaller arteries around the elbow joint. Anteriorly in the antecubital fossa, the brachial artery divides into the radial and ulnar arteries. The radial recurrent artery and the posterior and anterior ulnar recurrent arteries arise immediately beyond the origins of their respective arteries to form anastomoses with branches of the brachial and deep brachial arteries. The radial artery courses along the radial side of the forearm to the wrist, traverses the snuffbox, and turns medially to give rise to the deep palmar arch.”
CT Angiography of the Upper Extremity Arterial System: Part 1—Anatomy, Technique, and Use in Trauma Patients Bozlar U et al. AJR 2013; 201:745–752 - “Arterial injuries of the upper extremities occur in the setting of both blunt and penetrating trauma. Posttraumatic vascular abnormalities include spasm, external compression, dissection , occlusion or transection , arteriovenous fistula (AVF) development , pseudoaneurysm formation, rupture, and transection.”
CT Angiography of the Upper Extremity Arterial System: Part 1—Anatomy, Technique, and Use in Trauma Patients Bozlar U et al. AJR 2013; 201:745–752 - “In difficult cases, pseudoaneurysms can easily be differentiated from extravasation if late phase imaging is performed. Pseudoaneurysms maintain their shape and follow opacification characteristics of the aorta, whereas in arterial extravasation, contrast material spreads along tissue planes and has increased attenuation compared with parent arteries on delayed images.”
CT Angiography of the Upper Extremity Arterial System: Part 1—Anatomy, Technique, and Use in Trauma Patients Bozlar U et al. AJR 2013; 201:745–752 - “CTA is an important diagnostic imaging modality for the evaluation of upper extremity arterial abnormalities. High-quality CTA of the upper extremities is feasible on modern CT scanners using optimized scanning and con- trast injection technique. Its 24-hour availabil- ity, rapid acquisition, minimal invasiveness, and display of both vascular and musculoskeletal structures makes it particularly attrac- tive for the evaluation of patients with blunt or penetrating trauma to the upper extremity. .”
CT Angiography of the Upper Extremity Arterial System: Part 1—Anatomy, Technique, and Use in Trauma Patients Bozlar U et al. AJR 2013; 201:745–752 - “Arterial injuries included transection (24.3%), occlusion (17.3%), partial transection/flow limiting defect (24.5%), pseudoaneurysm (9.0%), and other injuries including intimal defects (22.7%). Nonoperative management was undertaken in 276 (50.9%), with failure in 4.0%. Definitive endovascular and open repair were used in 40 (7.4%) and 126 (23.2%) patients, respectively.”
The American Association for the Surgery of Trauma PROspective Observational Vascular Injury Treatment (PROOVIT) registry: multicenter data on modern vascular injury diagnosis, management, and outcomes. DuBose JJ et al. J Trauma Acute Care Surg. 2015 Feb;78(2):215-22 - “A total of 542 injuries from 14 centers (13 American College of Surgeons-verified Level I and 1 American College of Surgeons-verified Level II) have been captured since February 2013. The majority of patients are male (70.5%), with an Injury Severity Score (ISS) of 15 or greater among 32.1%.”
The American Association for the Surgery of Trauma PROspective Observational Vascular Injury Treatment (PROOVIT) registry: multicenter data on modern vascular injury diagnosis, management, and outcomes. DuBose JJ et al. J Trauma Acute Care Surg. 2015 Feb;78(2):215-22 - “Arterial injuries were categorized into 116 penetrating (73.0%) and 43 blunt (27.0%) mechanisms. Arterial distribution involved was as follows: 13 axillary (8.2%), 40 brachial (25.2%), 52 radial (32.7%), 51 ulnar (32.1%), and 3 other (1.9%). The types of arterial injuries were as follows: 69 transection (43.4%), 68 laceration (42.8%), 16 occlusion (10.1%), 3 avulsion (1.9%), and 3 entrapment (1.9%).”
A five-year review of management of upper-extremity arterial injuries at an urban level I trauma center. Franz RW et al. Ann Vasc Surg. 2012 Jul;26(5):655-64 - “One patient (0.7%) required a primary above-elbow amputation. The majority of injuries (96.8%) receiving vascular management underwent surgical intervention--76 primary repair (49.7%), 41 ligation (26.8%), 31 bypass (20.3%), and 5 endovascular (3.3%). Conservative treatment was the primary strategy for five arterial injuries (3.3%). Of the patients receiving vascular intervention, three (2.2%) required major and three (2.2%) required minor amputations during hospitalization and no patients expired.”
A five-year review of management of upper-extremity arterial injuries at an urban level I trauma center. Franz RW et al. Ann Vasc Surg. 2012 Jul;26(5):655-64 - “The current multidisciplinary team management approach with prompt surgical management resulted in successful outcomes after upper-extremity arterial injuries. No outcome differences between penetrating and blunt or between proximal and distal arterial injuries were calculated. This management approach will continue to be used.”
A five-year review of management of upper-extremity arterial injuries at an urban level I trauma center. Franz RW et al. Ann Vasc Surg. 2012 Jul;26(5):655-64 - “CT is the procedure of choice to identify hemorrhage, air, bullet, bone fragments, hemothorax, nerve lesion, musculoskeletal lesions, and vessels injuries and is useful for assessing medicolegal aspects as trajectory and the anatomical structures at risk.”
Imaging assessment of gunshot wounds. Reginelli A et al. Semin Ultrasound CT MR. 2015 Feb;36(1):57-67. - “Indication for total body computed tomography (CT) is based on the presence of signs and symptoms of vascular damage at clinical examination. Patients are immediately transferred in the operating room for surgery if more serious injuries that require immediate surgical care are not diagnosed, or hemostasis may be preliminary reached in the emergency room. Hemodynamically stable patients with no history and clinical examination showing suspected vascular damage are allowed in the radiology department for obtaining a total body CT scan with intravenous contrast medium and then transferred to the surgical ward trauma for observation.”
Imaging assessment of gunshot wounds. Reginelli A et al. Semin Ultrasound CT MR. 2015 Feb;36(1):57-67.
- “ CT angiography findings indicative of arterial injury were observed in 24 patients (30%) and a total of 43 arterial injuries were noted; the most common form was focal narrowing/spasm (n?=?16, 37.2%); the most common artery involved was the superficial femoral artery (n?=?12, 50%). In qualitative assessment of images based on a 4-point grading system, both readers considered CT angiography diagnostically excellent (grade 4) in most cases. Surgical findings were consistent with CT angiography and follow-up of patients' medical records showed no arterial injuries in patients with normal findings on initial imaging.”
Computed tomography angiography of lower extremities in the emergency room for evaluation of patients with gunshot wounds.
Adibi A et al.
Eur Radiol. 2014 Jul;24(7):1586-93 - “Our findings demonstrate that CT angiography is an effective imaging modality for evaluation of lower extremity gunshot wounds and could help limit more invasive procedures such as catheter angiography to a select group of patients.”
Computed tomography angiography of lower extremities in the emergency room for evaluation of patients with gunshot wounds.
Adibi A et al.
Eur Radiol. 2014 Jul;24(7):1586-93
- Vascular Emergencies of the Chest Post Trauma
- Aortic rupture (complete and incomplete)
- Traumatic aortic dissection
- Aortic dissection and rupture
- Traumatic acute intramural hematoma
- Pseudoaneurysm
- Catheter related injuries
- Foreign body embolization - “ Multirow CT angiography is a fast,safe and noninvasive imaging technique. In combination with two and three dimensional postprocessing techniques, it often clarifies complex vascular and nonvascular anatomy.”
Vascular Emergencies of the Thorax after Blunt and Iatrogenic Trauma: Multidetector Row CT and Three Dimensional Imaging
Alkadhi H et al.
RadioGraphics 2004:24:1239-1255
- Aortic Transection: Facts
- 10-20% of patients survive the initial event
- Occurs most commonly at aortic isthmus (space between brachiocephalic trunk and that of the ligamentum arteriosus)
- Mediastinal hematoma (anterior of posterior mediastinum) is common but not diagnostic of aortic injury
- Hematoma of interest most commonly around the aorta - Aortic Transection: Facts
- The direct signs of aortic transection include;
- Vessel caliber change
- Pseudoaneurysm
- Intramural flap - Cardiac Trauma: Differential Diagnosis
- Aortic transection
- Valvular rupture
- Hemopericardium
- Cardiac tamponade - Hypovolemic Shock: CT Findings
- Bright adrenals
- Diffuse fluid filled dilated small bowel
- Hyperenhancement of the small bowel
- Hyperenhancement of the gall bladder mucosa
- Reduced splenic perfusion
- Intense enhancement of the kidneys
- Peripancreatic edema
- Clinical Signs of Vascular Injury
Soft signs
- Significant hemorrhage found on history
- Decreased pulse compared to the contralateral extremity
- Bony injury or proximity to penetrating wound
- Neurologic abnormality - Arterial Injury: Patterns of Injury
- Hematoma
- Active extravasation
- Vasospasm
- Stenosis
- External compression
- Occlusion
- Intimal injury and dissection
- Arteriovenous fistulas
- Pseudoaneurysm formation - “ An advantage of 3D mapping is the ability to display the information in a format that not only simulates a classic catheter angiogram (digital subtraction), but also the capability to display tissue in addition to the vasculature,
including muscle, soft tissues, and bone. MIP
and VRT imaging may require segmentation with bone removal, especially when the extremities are involved. VRT is especially valuable when opaque foreign
matter is present.”
State of the art 3DCT angiography assessment of lower extremity trauma: typical findings, pearls and pitfalls
Fritz J, Efron DT, Fishman EK
Emerg Radiol (epub November 2012) - “A variety of factors may obscure or mimic vascular injury on MDCTA including inadequate arterial enhancement due to timing of the contrast injection, motion artifacts, inadequate positioning, streak artifacts, dense calcifications, and similar density of vessels and bone. Venous injuries may be missed on a single phase study or in the absence of late phase images.”
State of the art 3DCT angiography assessment of lower extremity trauma: typical findings, pearls and pitfalls
Fritz J, Efron DT, Fishman EK
Emerg Radiol (epub November 2012)
- AVFs or Arteriovenous Fistulas: Definition
-Arteriovenous Fistulas are abnormal communications with shunting of blood from am artery to a vein that mainly involve the peripheral vascular system but can affect virtually any organ or system in the body - Vascular Trauma: CT Findings Arterial injuries
- Pseudoaneurysm
- Active arterial hemorrhage
- AV fistulae
- Occlusion
- Intimal injury vasospasm "The use of multiphasic images affords more definitive characterization of areas of “contrast blush” as to the underlying etiologies of contained vascular injuries or active hemorrhage."
CT of Blunt Abdominal and Pelvic Vascular Injury
Vi M et al.
Emerg Radiol (2010) 17;21-29"Multiphasic imaging also allows for the definitive differentiation between arterial and venous sources of hemorrhage."
CT of Blunt Abdominal and Pelvic Vascular Injury
Vi M et al.
Emerg Radiol (2010) 17;21-29- CT Angiography: Potential Limitations in Extremity Trauma
- Inadequate arterial enhancement
- Motion artifact
- Inadequate positioning
- Streak artifact " By demonstrating the extent, location, and type of injury, CT angiography aids in the decision making process to determine the appropriate management for each injury in each patient."
Use of 64-Row Multidetector CT Angiography in Blunt and Penetrating Trauma of the Upper and Lower Extremities
Pieroni S et al.
RadioGraphics 2009; 29:863-876- Sixty-four-row multidetector CT angiography of the extremities has the ability to demonstrate a variety of vascular injuries such as occlusion, pseudoaneurysm, active extravasation, and intimal dissection."
Use of 64-Row Multidetector CT Angiography in Blunt and Penetrating Trauma of the Upper and Lower Extremities
Pieroni S et al.
RadioGraphics 2009; 29:863-876