Imaging Pearls ❯ Vascular ❯ Coronary Arteries
|
-- OR -- |
|
- “BBCR captures the cardiac valve anatomy and calcifications. CR has been used in the assessment of aortic valve variant anatomy, and BBCR improves the delineation of the valve cusps from the blood pool. Global valve and outflow tract calcification assessment can be challenging to fully capture on 2D imaging, and routine cinematic rendering displays often obscure the calcifications due to the opaque contrast-enhanced blood pool. BBCR has potential for the assessment of calcifications of the valve leaflets, annulus, and outflow tract in planning for transcatheter valve replacements .”
Expanded experience with cardiovascular black blood cinematic rendering.
Brookmeyer C, Chu LC, Rowe SP, Fishman EK.
Emerg Radiol. 2024 Apr;31(2):277-284. 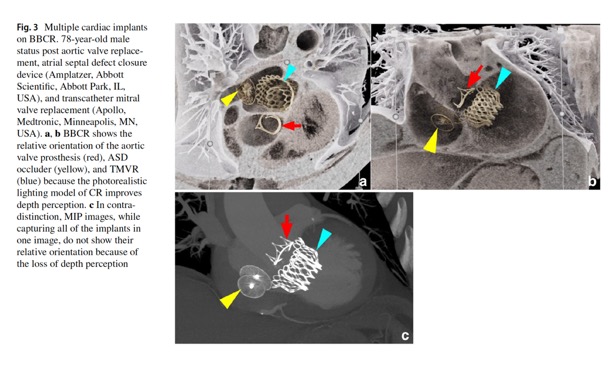
Expanded experience with cardiovascular black blood cinematic rendering.
Brookmeyer C, Chu LC, Rowe SP, Fishman EK.
Emerg Radiol. 2024 Apr;31(2):277-284.

- • Serial cardiac troponin (cTn) biomarkers, preferably high-sensitivity cardiac troponin (hs-cTn), are useful for rapid detection and exclusion of myocardial injury (class 1 strength of recommendation; level B-NR quality of evidence [nonrandomized]).
• Structured risk assessment and evidence-based clinical decision pathways(CDPs) should be used to facilitate disposition and guide diagnostic evaluation (class 1 strength; level B-NR quality).
• Low-risk patients with acute or stable chest pain may be discharged home without urgent cardiac testing (class 2a strength for acute chest pain, class 1 strength for stable chest pain; level B-R quality [randomized]).
Evaluation and Diagnosis of Chest Pain
David G. Beiser, Adam S. Cifu, Jonathan Paul
JAMA Published online July 1, 2022 - • For intermediate-risk patients with acute chest pain and no known coronary artery disease (CAD), coronary computed tomographic angiography (CCTA) is useful for exclusion of atherosclerotic plaque and obstructive CAD (class I strength; level A quality).
• For intermediate-risk patients with acute chest pain and no known CAD, functional testing (eg, exercise electrocardiography, stress echocardiography, stress positron emission tomography/single-photon emission computed tomography myocardial perfusion imaging, or stress cardiac magnetic resonance) is useful for diagnosis of myocardial ischemia (class I strength; level B-NR quality [nonrandomized]).
Evaluation and Diagnosis of Chest Pain
David G. Beiser, Adam S. Cifu, Jonathan Paul
JAMA Published online July 1, 2022 - • For intermediate-risk patients with acute chest pain and no known CAD, functional testing (eg, exercise electrocardiography, stress echocardiography, stress positron emission tomography/single-photon emission computed tomography myocardial perfusion imaging, or stress cardiac magnetic resonance) is useful for diagnosis of myocardial ischemia (class I strength; level B-NR quality[nonrandomized]).
• Clinically stable patients presenting with chest pain should be included in decision-making. Information about risk of adverse events, radiation exposure, costs, and alternative options should be provided to facilitate the discussion.
Evaluation and Diagnosis of Chest Pain
David G. Beiser, Adam S. Cifu, Jonathan Paul
JAMA Published online July 1, 2022
- “Coronary angiography is the current gold standard in providing anatomical information regarding the extent and severity of coronary artery disease. Access site practice has changed in a number of European and Asian countries from mainly being transfemoral (TFA) to transradial (TRA) in view of less access site related bleeding complications, mortality and shorter hospital stay associated with TRA. For instance, in the United Kingdom use of radial access has increased from 14% to 80% between 2005 and 2014 in patients undergoing percutaneous coronary intervention (PCI) and it is estimated that this practice change has saved an estimated 450 lives nationally.”
Hand dysfunction after transradial artery catheterization for coronary procedures
Muhammad Ayyaz Ul Haq et al.
World J Cardiol. 2017 Jul 26; 9(7): 609–619. - “Nevertheless, despite of its clear advantages over TFA, TRA is not without limitations and is associated with longer operator learning curve, increased radiation exposure in individual operators at the start of their learning curves and higher case radial proportion to translate the better results of randomized trials into clinical practice. Moreover, vascular complications such as RAO and radial artery spasm are not uncommon and very recently concerns have been raised that patients undergoing TRA PCI may encounter hand dysfunction.”
Hand dysfunction after transradial artery catheterization for coronary procedures
Muhammad Ayyaz Ul Haq et al.
World J Cardiol. 2017 Jul 26; 9(7): 609–619. - “In conclusion, hand dysfunction is an exceedingly rare complication post TRA. There is significant heterogeneity in the methodology and reporting of the studies investigating hand function after TRA. Patients may develop non-specific sensory symptoms or muscle weakness but majority of these symptoms resolve over time. Future studies should be focused around assessing such complications using robust methodology and more importantly reporting on the clinical relevance of hand function. Given the reductions in mortality, MACE and major bleeding complications associated with use of TRA in high risk groups undergoing PCI, TRA should remain the default access site for PCI in such high risk groups of patients at risk of bleeding complications, in line with international guidelines and consensus statements.”
Hand dysfunction after transradial artery catheterization for coronary procedures
Muhammad Ayyaz Ul Haq et al.
World J Cardiol. 2017 Jul 26; 9(7): 609–619. - “ Coronary artery dissection with aortic extension can be a fatal although infrequent complication. he coronary artery entry point is usually stented in the catherization laboratory. Thereafter, CT is the imaging modality of choice for immediate confirmation of the presence or residual iatrogenic dissection and evaluation of its extent and later noninvasive follow-up.”
Catheter Induced Aortic Dissection After Invasive Coronary Angiography: Evaluation With MDCT
Tanasie C et al.
AJR 2011;197:1335-1340 - “ CT is a powerful diagnostic tool for evaluating the pericardium and its abnormalities. Knowledge of the normal recesses and sinuses is essential to avoid misdiagnosis. Functional imaging is useful in the evaluation of pricardial constriction and tamponade.”
Computed Tomography of the Pericardium and Pericardial Disease
Rajiah P et al.
J Cardiovasc Comput Tomogr (2010) 4,3-18 - Normal Pericardium: Facts
- < 2 mm thick
- Contains 15-50 ml of fluid
- Pericardial recesses can be confused with adenopathy or other masses - Cardiac Tamponade: CT Findings
- Large pericardial effusion
- Enlargement of either the SVC (diameter similar or greater than adjacent aorta) or IVC (diameter twice adjacent aorta)
- Periportal edema
- Reflux of contrast into IVC and azygous vein or enlargement of hepatic and renal veins - “Coronary artery anastomotic dehiscence is a rare complication following aortic root repair in Marfan's disease. In this patient who presented several years after surgery with mediastinal and chest wall hematoma, gated IV contrast enhanced cardiac CT was able to noninvasively localize left main coronary artery anastomotic dehiscence as the source of bleeding.”
Dehiscence of coronary artery graft presenting as a right breast mass
Samet JD, Johnson PT, Fishman EK Cardiovasc Comput Tomogr. 2011 May-Jun;5(3):180-2 - “Currently, there are two main types of surgical correction, the Bentall procedure or composite graft with aortic valve replacement, and aortic valve-sparing. Both procedures have low operative risk. Since a prosthetic valve is used in the Bentall procedure, it is associated with higher rates of thromboembolism, and thus these patients must be anti-coagulated. The valve-sparing procedure has lower rates of thromboembolism given the native aortic valve, but re-operation rates have been shown to be higher than the Bentall procedure. Patients who undergo the Bentall procedure have lower late survival rates, but this is likely due to its preferred use in emergent higher risk cases.”
Dehiscence of coronary artery graft presenting as a right breast mass
Samet JD, Johnson PT, Fishman EK Cardiovasc Comput Tomogr. 2011 May-Jun;5(3):180-2 - "The optimal reconstruction phase varied between patients, and this was directly related to the heart rate. For patients with a heart rate of 70 beats per minute, the reconstruction phase centered at 75% of the R-R interval had the significantly least motion artifact. Conversely the optimal reconstruction phase for patients with heart rates above 70 beat per minute was centered at 50% of the R-R interval."
- "The optimal reconstruction phase varied between patients, and this was directly related to the heart rate."
Thoracic Aorta at Multidetector Row CT: Motion Artifact with Various Reconstruction Windows
Morgan-Hughes GJ et al.
Radiology 2003; 228:583-588