Imaging Pearls ❯ Contrast ❯ Catheters
|
-- OR -- |
|
- OBJECTIVE. The purpose of this study was to assess the difference between mechanical versus hand administration of IV contrast agents on the diagnostic quality of pediatric pulmonary CT angiography (CTA).
CONCLUSION. It is possible to perform diagnostic-quality pulmonary CTA for the assessment of the central pulmonary arteries with hand administration of IV contrast material in pediatric patients with small-gauge IV catheters.
Comparison of Mechanical Versus Hand Administration of IV Contrast Agents for Pediatric Pulmonary CT Angiography Zapala MA et al. AJR 2017; 208:632–636 - “For pediatric patients, pulmonary CTA has become a mainstay for a variety of indications, including pulmonary embolism, pulmonary sling, pulmonary artery hypertension, and pre-or postoperative lung transplants. Pulmonary CTA offers advantages over traditional catheter-based angiography and nuclear medicine ventilation-perfusion studies in terms of improved speed, wider availability, increased contrast and spatial resolution, postprocessing abili- ties, and assessment of other structures outside of the vasculature.”
Comparison of Mechanical Versus Hand Administration of IV Contrast Agents for Pediatric Pulmonary CT Angiography Zapala MA et al. AJR 2017; 208:632–636 - “In conclusion, hand administration of IV contrast material in young children (≤ 5 years) and infants when used in conjunction with a bolus-tracking method yields diagnostic- quality pulmonary CTA studies. This study supports practicing radiologists in the use of hand administration of IV contrast material for pulmonary CTA studies when young children have IV access locations and sizes that preclude mechanical administration.”
Comparison of Mechanical Versus Hand Administration of IV Contrast Agents for Pediatric Pulmonary CT Angiography Zapala MA et al. AJR 2017; 208:632–636
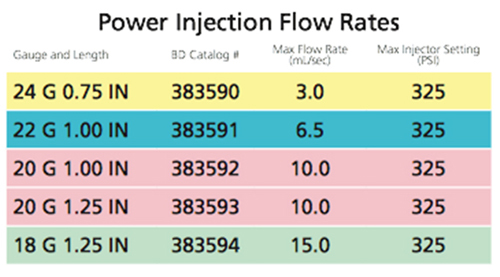
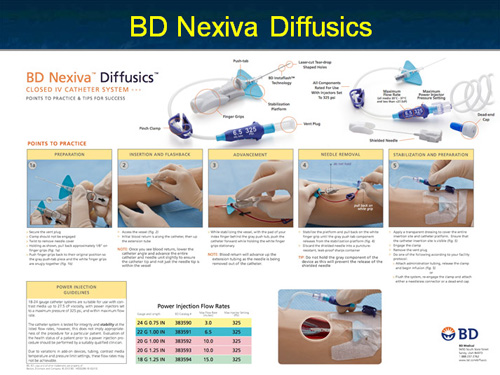
- The BD Nexiva™ Diffusics™ System: Advantages
• Reduces the destabilizing effects that can lead to extravasation
• Catheter tip features multiple teardrop-shaped diffusion holes to reduce forces that cause catheter motion in the vein by up to 67%*
• Enable high flow rates with patients that may require a smaller IV catheter
• Enables higher flow rates with a smaller gauge catheter (22 G - 24 G),* facilitating difficult venous access situations
- “OBJECTIVE. The purpose of this study was to evaluate the effectiveness of various contrast injection sites when performing thoracic CT angiography (CTA) using hand injection of IV contrast material in infants and young children with a small IV catheter.
CONCLUSION. Diagnostic quality thoracic CTA can be achieved with hand injection of IV contrast material in infants and young children with a small IV catheter, independent of the IV access site.”
Evaluation of Contrast Injection Site Effectiveness: Thoracic CT Angiography in Children With Hand Injection of IV Contrast Material
Gary R. Schooler GR et al.
AJR 2015 204:2, 423-427 - “Six individual injection sites were identified: head, jugular vein, arm vein, hand vein, leg vein, and foot vein. Injection sites were categorized into three regional groups: head-neck region (head vein and jugular veins), upper extremity region (arm and hand veins), and lower extremity region (leg and foot veins). Comparisons of attenuation values between individual and regionally grouped contrast injection sites were determined using the F-test in ANOVA.”
Evaluation of Contrast Injection Site Effectiveness: Thoracic CT Angiography in Children With Hand Injection of IV Contrast Material
Gary R. Schooler GR et al.
AJR 2015 204:2, 423-427
- “In the ICU, peripherally inserted central catheters (PICCs) may be an alternative option to standard central venous catheters, particularly in patients with coagulation disorders or at high risk for infection. Some limits of PICCs (such as low flow rates) may be overcome with the use of power-injectable catheters.”
Clinical experience with power-injectable PICCs in intensive care patients.
Pittiruti M et al.
Crit Care. 2012 Feb 4;16(1):R21. - “ Power-injectable PICCs have many advantages in the ICU: they can be used as multipurpose central lines for any type of infusion including high-flow infusion, for hemodynamic monitoring, and for high-pressure injection of contrast media during radiological procedures. Their insertion is successful in 100% of cases and is not associated with significant risks, even in patients with coagulation disorders. Their maintenance is associated with an extremely low rate of infective and non-infective complications.”
Clinical experience with power-injectable PICCs in intensive care patients.
Pittiruti M et al.
Crit Care. 2012 Feb 4;16(1):R21. - “The purpose of this study was to compare the performance of a 20-gauge fenestrated catheter with an 18-gauge nonfenestrated catheter for i.v. contrast infusion during MDCT.”
I.v. contrast administration with dual source 128-MDCT: a randomized controlled study comparing 18-gauge nonfenestrated and 20-gauge fenestrated catheters for catheter placement success, infusion rate, image quality, and complications.
Johnson PT, Christensen GM, Fishman EK.
AJR Am J Roentgenol. 2014 Jun;202(6):1166-70. - “A 20-gauge fenestrated catheter performs similarly to an 18-gauge nonfenestrated catheter with respect to i.v. contrast infusion rates and aortic enhancement levels and can be placed in most subjects whose veins are deemed insufficient for an 18-gauge catheter.”
I.v. contrast administration with dual source 128-MDCT: a randomized controlled study comparing 18-gauge nonfenestrated and 20-gauge fenestrated catheters for catheter placement success, infusion rate, image quality, and complications.
Johnson PT, Christensen GM, Fishman EK.
AJR Am J Roentgenol. 2014 Jun;202(6):1166-70.

- “ This study evaluated the effect of intravenous (IV) catheter gauge size on catheter placement, contrast infusion, and image quality for patients undergoing IV contrast-enhanced multidetector computed tomography (MDCT).”
Catheter insertion for intravenous (IV) contrast infusion in multidetector-row computed tomography (MDCT): defining how catheter caliber selection affects procedure of catheter insertion, IV contrast infusion rate, complication rate, and MDCT image quality.
Johnson PT, Christensen G, Lai H, Eng J, Fishman EK.
J Comput Assist Tomogr. 2014 Mar-Apr;38(2):281-4 - “Experienced IV starters usually achieve IV access in one attempt by tailoring IV catheter gauge to vein quality; however, target infusion rates are not likely to be achieved with 22- and 24-gauge catheters, used in nearly 1/3 of the patients in this study.”
Catheter insertion for intravenous (IV) contrast infusion in multidetector-row computed tomography (MDCT): defining how catheter caliber selection affects procedure of catheter insertion, IV contrast infusion rate, complication rate, and MDCT image quality.
Johnson PT, Christensen G, Lai H, Eng J, Fishman EK.
J Comput Assist Tomogr. 2014 Mar-Apr;38(2):281-4



- “A 20-gauge fenestrated catheter performs similarly to an 18-gauge nonfenestrated catheter with respect to i.v. contrast infusion rates and aortic enhancement levels and can be placed in most subjects whose veins are deemed insufficient for an 18-gauge catheter.”
I.V. contrast administration with dual source 128-MDCT: a randomized controlled study comparing 18-gauge nonfenestrated and 20-gauge fenestrated catheters for catheter placement success, infusion rate, image quality, and complications
Johnson PT, Christensen GM, Fishman EK
AJR Am J Roentgenol. 2014 Jun;202(6):1166-70 - “For image quality and safety purposes, when the infusion rate exceeds 5mL/s, IV contrast material is ideally delivered through an 18-gauge peripheral venous catheter. However, not all patients have venous access that can accommodate an 18-gauge catheter, particularly oncology patients.”
I.V. contrast administration with dual source 128-MDCT: a randomized controlled study comparing 18-gauge nonfenestrated and 20-gauge fenestrated catheters for catheter placement success, infusion rate, image quality, and complications
Johnson PT, Christensen GM, Fishman EK
AJR Am J Roentgenol. 2014 Jun;202(6):1166-70 - “ In light of the trend toward faster contrast infusion in practice, fenestrated catheters have the capacity to expand the population of patients who can be imaged safely with the required rapid IV contrast infusion rates and thus benefit from optimal enhancement quality.”
I.V. contrast administration with dual source 128-MDCT: a randomized controlled study comparing 18-gauge nonfenestrated and 20-gauge fenestrated catheters for catheter placement success, infusion rate, image quality, and complications
Johnson PT, Christensen GM, Fishman EK
AJR Am J Roentgenol. 2014 Jun;202(6):1166-70 - “To assess current practice of United Kingdom cardiologists with respect to patients with reported shellfish/iodine allergy, and in particular the use of iodinated contrast for elective coronary angiography. Moreover we have reviewed the current evidence-base and guidelines available in this area.”
Shellfish allergy and relation to iodinated contrast media: United Kingdom survey.
World J Cardiol. 2014 Mar 26;6(3):107-11
Baig M et al.
- IV Catheter Safety
- Most IV catheters are pressure rated and usually the safety on the injector is for a pressure of 300 psi or less. Exceeding this can result in product leakage and or damage to the catheter and potentially injury to the patient
- Some of the newer generation IV catheters like the BD Nexiva Diffusics can be used to a psi of 325
- Please be certain that you are aware of what catheter you use and in practice it is ideal to use one brand only to prevent errors in setting the psi values in routine practice - “ After the intervention, mean ED LOS among oral contrast eligible patients decreased by 97 min. Mean time from order to CT decreased by 66 minutes. No patient with CT Negative for acute findings had additional subsequent AP imaging within 72 h at our institution that led to a change in diagnosis.”
Eliminating routine oral contrast use for CT in the emergency department: impact on patient throughput and diagnosis
Levenson RB et al.
Emerg Radiol (2012) 19:513-517 - “ Eliminating routine oral contrast use for AP CT in the ED may be successful in decreasing LOS and time from order to CT without demonstrated compromise in acute patient diagnosis.”
Eliminating routine oral contrast use for CT in the emergency department: impact on patient throughput and diagnosis
Levenson RB et al.
Emerg Radiol (2012) 19:513-517