|
-- OR -- |
|
- The applications of AI for imaging of CAD using CT span multiple arenas including plaque detection, plaque characterization, improving risk stratification, and clinical decision-making. AI has been applied to both CAC scoring and CCTA. Studies have shown the ability of AI to detect hemodynamically significant stenosis across a broad range of imaging parameters and its potential ability to decrease the time needed for analysis of images for stenosis. AI can significantly reduce the time to perform quantitative plaque analysis, an important barrier to its application in clinical practice.
Coronary Artery Disease: Role of Computed Tomography and Recent Advances
Elizabeth Lee et al
Radiol Clin N Am - (2024 (in press) - “One trial of AI-based CCTA interpretation in patients with stable chest pain referred for ICA found a lower cost compared with conventional interpretation due to lower rates of referral for ICA, without impacting the occurrence of cardiac events. A comprehensive review of all potential applications for AI in CT imaging of CAD is beyond the scope of this review; however, AI is certain to change how imaging is ordered, performed, and interpreted in the near future.”
Coronary Artery Disease: Role of Computed Tomography and Recent Advances
Elizabeth Lee et al
Radiol Clin N Am - (2024 (in press) - • Coronary computed tomography angiography (CCTA) has the highest level of evidence supporting its use in patients with acute and stable chest pain.
• CCTA can identify high-risk plaque features and quantify overall plaque burden, providing important prognostic information which has been incorporated into CADRADS 2.0.
• In asymptomatic patients, currently, there is no evidence for the use of CCTA; however, ongoing trials aim to determine whether CCTA can provide additional prognostic information above those from coronary calcium scoring and clinical risk factors.
Coronary Artery Disease: Role of Computed Tomography and Recent Advances
Elizabeth Lee et al
Radiol Clin N Am - 2024 (in press)
- Multiple Coronary Artery Aneurysms: Differential Dx
- Atherosclerosis
- Kawasaki disease
- Takayasu's arteritis and polyarteritis nodosa
- infections (such as narcotic emboli, syphilis, and Lyme disease),
- cocaine abuse - “Patients are often asymptomatic when they are diagnosed with coronary aneurysms, but they may present with exercise-induced angina, unstable angina, and, occasionally, myocardial infarction. Potential complications include thrombosis, embolism, rupture, fistula to the cardiac chambers, and endocarditis. Most giant coronary aneurysms reported in the medical literature have involved the RCA adjacent to the right atrium.”
Multiple giant coronary artery aneurysms.
Marla R, Ebel R, Crosby M, Almassi GH.
Tex Heart Inst J. 2009;36(3):244-6. PMID: 19568397; PMCID: PMC2696511. - Coronary artery aneurysm (CAA) is a rare pathology of the coronary arteries and is present in up to 4.9% of patients undergoing coronary angiography. Although a consensus classification of CAA is lacking, CAA is generally defined as dilations of the coronary artery where the diameter of the distended segment is 150% of the diameter of the adjacent segments. Furthermore, CAA can be termed “giant” if the dilated segment is either > 8 mm in diameter or 400% of the diameter of the adjacent segments. Among those patients with CAA, dilation of the right coronary artery (RCA) is the most common aneurysmal finding followed by dilation of the left anterior descending coronary artery (LAD). Concomitant aneurysms of both the RCA and the LAD are extraordinarily rare, and when present, are most frequently associated with Kawasaki disease.
Giant coronary artery aneurysms involving more than one coronary artery: case report.
Khouzam, M.S., Khouzam, N.
J Cardiothorac Surg 16, 177 (2021). - “Concomitant aneurysms of both the RCA and the LAD are extraordinarily rare, and when present, are most frequently associated with Kawasaki disease.”
Giant coronary artery aneurysms involving more than one coronary artery: case report.
Khouzam, M.S., Khouzam, N.
J Cardiothorac Surg 16, 177 (2021). - Coronary Artery Aneurysm: Facts
- Coronary artery aneurysm (CAA) is a rare pathology of the coronary arteries and is present in up to 4.9% of patients undergoing coronary angiography.
- Although a consensus classification of CAA is lacking, CAA is generally defined as dilations of the coronary artery where the diameter of the distended segment is 150% of the diameter of the adjacent segments. Furthermore, CAA can be termed “giant” if the dilated segment is either > 8 mm in diameter or 400% of the diameter of the adjacent segments.
- dilation of the right coronary artery (RCA) is the most common aneurysmal finding followed by dilation of the left anterior descending coronary artery (LAD).
- Atherosclerosis is the most common cause of coronary aneurysms in North America and Europe, accounting for more than 50% of the cases. Other causes include Kawasaki disease, other vasculitides (such as Takayasu's arteritis and polyarteritis nodosa), lupus erythematosus, connective tissue disorders, congenital defects, infections (such as narcotic emboli, syphilis, and Lyme disease), trauma, dissection, cocaine abuse, and iatrogenic and idiopathic origins
- Coronary Artery Aneurysms
- Atherosclerosis
- Kawasaki disease, other vasculitides (such as Takayasu's arteritis and polyarteritis nodosa)
- lupus erythematosus
- connective tissue disorders
- congenital defects
- infections (such as narcotic emboli, syphilis, and Lyme disease)
- trauma
- dissection,
- cocaine abuse
- iatrogenic and idiopathic origins
- Degree of luminal diameter stenosis
-- 0% No visible stenosis
-- 1–24% Minimal stenosis
-- 25–49% Mild stenosis
-- 50–69% Moderate stenosis
-- 70–99% Severe stenosis
-- 100% Occluded - “Despite the robust evidence base supporting the use of CCTA in patients with acute and stable chest pain, there is insufficient prospective randomized clinical trial data to support the optimal clinical management strategy following CCTA. Accordingly, the CAD-RADS classification is an expert consensus document. As such, the recommendations provided in this document are based on the available research data from clinical trials as well as on broad expert consensus. This includes the suggested categories for reporting and the recommendations for further patient management, which need to be interpreted in the context of other available clinical information for each individual patient.”
CAD-RADS 2.0 – 2022 Coronary Artery Disease – Reporting and Data System.
Ricardo C. Cury, Jonathon Leipsic, Suhny Abbara et al.
J Am Coll Radiol 2022;19:1185-1212
- Coronary Artery Aneurysms: Causes
- Atherosclerotic disease
- Vasculitis (Kawasaki Disease, Takayasu Disease, PAN)
- Connective Tissue Disease (Marfans, Ehlers-Danlos disease)
- Infection (Bacterial, mycobacterial, fungal, Lyme disease)
- IVDA (cocaine, amphetamines)
- Congenital (FMD) - “Appendix 1 lists various causes of coronary artery aneurysms. Categories include atherosclerotic disease, unusual vascular conditions (Kawasaki disease, Takayasu aortitis), and genetic syndromes (Loeys-Dietz syndrome) . More appropriately defined as pseudoaneurysms are aneurysms resulting from iatrogenic or traumatic causes (cardiac catheterization, surgery and from infectious processes. In the United States, atherosclerosis is the most common cause for coronary artery aneurysm disease; however, Kawasaki disease is the most common cause worldwide.”
CT Angiography of Coronary Artery Aneurysms: Detection, Definition, Causes, and Treatment
Pamela T. Johnson, Elliot K. Fishman
AJR 2010; 195:928–934
- “Furthermore, three-dimensional volume-rendered CT angiograms facilitate accurate assessment of the complex anatomy of CAFs, including their origin, drainage site, and complexity and the number and size of fistulous tracts. Knowledge of these characteristics is crucial for therapeutic planning.”
Coronary Artery Fistulas: Pathophysiology, Imaging Findings, and Management
Yum G, Nam Th, Chun EJ
RadioGraphics 2018; 38:688–703 - “Although CAFs historically have been evaluated with conventional invasive angiography,electrocardiographically gated cardiac computed tomographic (CT) angiography has emerged as the noninvasive alternative modality of choice owing to the high spatial and temporal resolution and short acquisition time. Furthermore, three-dimensional volume-rendered CT angiograms facilitate accurate assessment of the complex anatomy of CAFs, including their origin, drainage site, and complexity and the number and size of fistulous tracts. Knowledge of these characteristics is crucial for therapeutic planning.”
Coronary Artery Fistulas: Pathophysiology, Imaging Findings, and Management
Yum G, Nam Th, Chun EJ
RadioGraphics 2018; 38:688–703 - Coronary Artery Fistulae: Clinical Presentation
- Incidental finding
- myocardial ischemia
- heart failure
- arrhythmia
- infective endocarditis in adults - “A coronary artery fistula (CAF) or coronary arteriovenous fistula is a congenital or acquired abnormal vascular communication of coronary arteries with cardiac chambers or any segment of the systemic or pulmonary circulation, without an intervening capillary network.”
Coronary Artery Fistulas: Pathophysiology, Imaging Findings, and Management
Yum G, Nam Th, Chun EJ
RadioGraphics 2018; 38:688–703 - “The drainage site of a CAF is more important clinically than the origin. A shunt to low-pressure structures may dilate the coronary arteries and sometimes lead to aneurysm formation.”
Coronary Artery Fistulas: Pathophysiology, Imaging Findings, and Management
Yum G, Nam Th, Chun EJ
RadioGraphics 2018; 38:688–703 - Coronary Artery Fistulae: Etiology
- Congenital (90%)
- Acquired (10%)
-- coronary stent placement
-- coronary bypass surgery
-- trauma
-- chest irradiation
-- myocardial infarction - Coronary Artery Fistulae: Facts
- The right coronary artery (RCA) is the most common origin site of CAFs, accounting for 50%–55% of cases.
- The left anterior descending artery (LAD), accounting for about 35%–40% of cases
- left circumflex artery, accounting for 5%–20% cases - Coronary Artery Fistulae: Facts
- The drainage site of CAFs is more important clinically than the origin and is classified into two fistula categories: coronary cameral fistulas, with which coronary arteries drain into the cardiac chamber, and coronary arteriovenous fistulas, with which coronary arteries drain into any segments of the pulmonary or systemic circulation - Coronary Artery Fistulae: Facts
- Coronary cameral fistula, defined as the entry of a coronary artery into any of the cardiac chambers, is considered the most common type of CAF detected with coronary angiography. Coronary cameral fistulas commonly originate from the RCA (55%), the LAD (35%), or both of these arteries.The most commonly involved chamber is the right ventricle (41%), followed by the right atrium (26%) and the left atrium and left ventricle (3%–5%) - Coronary Artery Fistulae: Facts
- The incidence of coronary-to-pulmonary artery fistulas has increased as cardiac CT angiography has become widely used, with these fistulas accounting for 15%–30% of all CAFs
- results of a recent systematic review (41) showed the LCA to be the most common origin site (84% of cases), followed by the RCA (38% of cases). The majority (89%) of CAFs drain into the pulmonary trunk rather than into other segmental pulmonary arteries. - Coronary Artery Fistulae: Management
- Percutaneous transcatheter closure
-- Proximal fistula origin
-- Single drain site
-- Nontortuous vessel with distal portion of fistula accessible with the closure device
-- Extra-anatomic termination of fistula away from normal coronary arteries
-- Older patients with high risk of perioperative complications
-- Absence of concomitant cardiac disorders - Coronary Artery Fistulae: Management
- Surgical ligation
-- Large symptomatic fistula with high fistula blood flow
-- Multiple communications and drainage sites
-- Tortuous and aneurysmal fistulous arteries
-- Need for simultaneous distal bypass
-- Large vascular branches that can be accidentally embolized - “A CAF is a rare anomaly with a variable clinical course, from no symptoms to serious complications that include heart failure and myocardial infarction—depending on the extent of the shunt. ECG-gated CT angiography with 3D reconstruction can be used to accurately assess the complex anatomy of CAFs, including the site and number of origins and drainage sites, and the associated anomalies. This information is essential for therapeutic planning.”
Coronary Artery Fistulas: Pathophysiology, Imaging Findings, and Management
Yum G, Nam Th, Chun EJ
RadioGraphics 2018; 38:688–703 - “Coronary–pulmonary artery fistula in adults was found more often than in previous studies. CAF commonly originates from LCA or both LCA and RCA in adults. DSCT is a robust tool for investigating the origin, course and drainage site of CAF and coexistent abnormalities.”
Coronary artery fistula in adults: evaluation with dual- source CT coronary angiography
ZHOU K et al.
Br J Radiol 2015;88:20140754. - “DSCT could provide motion-free high-resolution images by using an electrocardiographically gated technique, especially for coronary CTA with complex vascular anatomy, despite the limited haemodynamic information. The multiplanar reformation can clearly demonstrate the sites of origin and termination of abnormal blood vessels, and the volume-rendered images acquired from three-dimensional CT data sets can provide an overview of the heart as well as its vascular anatomy and help surgeons to understand the anatomical complexity before surgery.”
Coronary artery fistula in adults: evaluation with dual- source CT coronary angiography
ZHOU K et al.
Br J Radiol 2015;88:20140754. - Coronary Artery Fistulae: Associated Findings
- tetralogy of Fallot,
- atrial septal defects,
- patent ductus arteriosus
- ventricular septal defects
- pulmonary atresia with an intact ventricular septum - “With advances in technology, computed tomography coronary angiography (CTCA) can be developed as a low-radiation imaging paradigm for children with KD.7-10 Advantages over echocardiography include the ability to visualize middle and distal coronary segments with little or no interobserver variability. Unlike catheter angiography, CTCA is noninvasive and clearly delineates intramural abnormalities. Besides, the measurements of coronary artery abnormalities (CAA) on catheter angiography.”
Computed Tomography Coronary Angiography for Evaluation of Children With Kawasaki Disease
Manphool Singhal et al.
Current Problems in Diagnostic Radiology 47 (2018) 238–244 - "In KD, any segment of coronary arteries and their major branches can be involved, although the majority of aneurysms occur in proximal segments. On echocardiography, it is difficult to evaluate middle and distal segments of coronary arteries, particularly in older children. Besides, CTCA is superior to echocardiography in In KD, any segment of coronary arteries and their major branches can be involved, although the majority of aneurysms occur in proximal segments. On echocardiography, it is difficult to evaluate middle and distal segments of coronary arteries, particularly in older children. Besides, CTCA is superior to echocar- diography in the assessment of coronary stenoses and calcifications.”
Computed Tomography Coronary Angiography for Evaluation of Children With Kawasaki Disease
Manphool Singhal et al.
Current Problems in Diagnostic Radiology 47 (2018) 238–244 - “In conclusion, high-risk patients with histories of KD had nonobstructive and obstructive CAD not visualized by other noninvasive imaging tests. In properly selected high-risk patients with KD, coronary CTA may identify a subset at increased risk for future coronary pathology who may benefit from medical therapy.”
Coronary Computed Tomographic Angiographic Findings in Patients With Kawasaki Disease
Kelly Han B, Lesser A, Rosenthal K et al.
Am J Cardiol 2014;114:1676e1681 - “We identified obstructive and nonobstructive CAD by coronary CTA in a highly select group of patients with KD with acute-phase coronary artery dilatation, resolved coronary aneurysms, or persistent coronary aneurysms. Coronary disease was present at the time of coronary CTA, with and without persistent coronary aneurysms. Stress imaging studies rarely suggested the presence of physiologically important CAD in those with or without obstruction.”
Coronary Computed Tomographic Angiographic Findings in Patients With Kawasaki Disease
Kelly Han B, Lesser A, Rosenthal K et al.
Am J Cardiol 2014;114:1676e1681 - Coronary Artery Aneurysms: Facts
- Hereditary connective tissue disorders like Marfan syndrome and Ehlers–Danlos disease can also result in CAAs.
- Bacterial, mycobacterial, fungal, syphilitic, Lyme, septic emboli, mycotic aneurysm, and HIV infections are also different CAA etiologies. - “The management of CAAs remains a clinical challenge and should be tailored to each patient based on a comprehensive clinical evaluation that encompasses the patient’s cardiovascular risk factors, comorbidities, and the nature and anatomy of the CAA to enable a patient-specific treatment plan. Certainly, as the understanding of the pathophysiology and etiology of CAAs develops, the treatment and prognosis of CAAs will improve.”
Coronary Artery Aneurysms: A Review of the epidemiology, Pathophysiology, Diagnosis, and Treatment
Sherif SA et al.
Frontiers in Cardiovascular Medicine May 2017 Vol 4; 1-12 - “The management of CAAs remains a clinical challenge and should be tailored to each patient based on a comprehensive clinical evaluation that encompasses the patient’s cardiovascular risk factors, comorbidities, and the nature and anatomy of the CAA to enable a patient-specific treatment plan. Certainly, as the understanding of the pathophysiology and etiology of CAAs develops, the treatment and prognosis of CAAs will improve.”
Coronary Artery Aneurysms: A Review of the epidemiology, Pathophysiology, Diagnosis, and Treatment
Sherif SA et al.
Frontiers in Cardiovascular Medicine May 2017 Vol 4; 1-12 - Coronary Artery Aneurysms: Etiologies
- Atherosclerosis,
- Takayasu arteritis,
- Congenital disorders,
- Kawasaki disease (KD)
- Percutaneous coronary intervention
- Trauma
- Ehlers Danlos Syndrome
- Marfans Syndrome - Coronary Artery Aneurysms: Facts
- Incidence higher in men than in woman (2.2% vs 0.5%)
- Right coronary artery most commonly affected and is involved in 40-70% of cases
- most common cause of CAAs is atherosclerosis, which has been linked to 50% of CAAs diagnosed in adults - Coronary Artery Aneurysms: Facts
Kawasaki disease is the most common cause of CAAs in childhood and is the second most common cause in adults. KD is an acute inflammatory syndrome that may result in acute vasculitis of the coronary arteries and subsequent coronary artery dilatation and aneurysm formation; CAAs occur in around 10–15% of patients during the acute phase of the disease - “Kawasaki’s disease (KD) is a vasculitis that predominantly affects children and can lead to the development of coronary artery aneurysms. These aneurysms can subsequently thrombose and occlude, which may lead to chest pain and other signs and symptoms of acute coronary syndrome in young patients. Coronary CT angiography, including 3D visualization techniques, is a common modality used in the follow-up of KD patients.”
Evaluation of Kawasaki’s disease-associated coronary artery aneurysms with 3D CT cinematic rendering
Rowe SP, Zimmerman SL, Johnson PT, Fishman EK
Emergency Radiology (2018) 25:449–453 - “The most important potential complication of KD is in- flammatory damage to the coronary arteries, which classically leads to the formation of coronary artery aneurysms. These aneurysms will often undergo vascular remodeling and partial thrombosis in order to produce a psuedonormal vascular lumen. However, progressive thrombosis and other stenotic processes such as fibrosis can, over time, precipitate cardiac ischemia that can lead to emergency room presentations for chest pain or other signs of acute coronary syndrome and necessitate invasive and/or surgical interventions.”
Evaluation of Kawasaki’s disease-associated coronary artery aneurysms with 3D CT cinematic rendering
Rowe SP, Zimmerman SL, Johnson PT, Fishman EK
Emergency Radiology (2018) 25:449–453
- Coronary Artery to Pulmonary Artery Fistulae Involving both the LAD and RCA
● cinematic rendering makes use of a more complex lighting model that creates photorealistic images with improved detail and that demonstrate shadowing effects that allow for robust visualization of the relative positions of structures - "Cinematic rendering (CR) a new method of 3D computed tomography (CT) volumetric visualization that produces photorealistic images. As with traditional 3D visualization methods, CR may prove to be of value in providing important information when evaluating regions of complex anatomy such as the heart."
Cinematic rendering of cardiac CT volumetric data: Principles and initial observations
Rowe SP, Johnson PT, Fishman EK
J Cardiovasc Comput Tomogr. 2018 Jan - Feb;12(1):56-59. - "Appropriate selection of window presets using either a ramp (for tissues differing markedly in attenuation such as bone in comparison to adjacent soft tissue) or trapezoid method (for differentiation of similar attenuation structures such as adjacent soft tissues) and slab thickness will allow for appropriate display of pathology and will ensure that a finding of interest is not obscured by an overlying structure."
Cinematic rendering of cardiac CT volumetric data: Principles and initial observations
Rowe SP, Johnson PT, Fishman EK
J Cardiovasc Comput Tomogr. 2018 Jan - Feb;12(1):56-59. - "While the shadowing effects that arise from the global lighting model that is used contribute to the photorealistic quality of the images, shadowing can also potentially obscure important pathology."
Cinematic rendering of cardiac CT volumetric data: Principles and initial observations
Rowe SP, Johnson PT, Fishman EK
J Cardiovasc Comput Tomogr. 2018 Jan - Feb;12(1):56-59.
- " CR differs from traditional VR in making use of a global lighting model that more realistically takes into account the interactions of propagating photons with the component materials of the imaged volume. As a result, this method enhances surface detail and creates lifelike shadowing effects in order to generate truly photorealistic visualizations from standard CT acquisition volumetric data. "
Evaluation of Kawasaki’s disease-associated coronary artery aneurysms with 3D CT cinematic rendering
Rowe SP, Zimmerman SL, Johnson PT, Fishman EK
Emergency Radiology (2018) 25:449–453 - In this case series, we have demonstrated the ability of CR visualizations to effectively convey key anatomic information related to coronary artery aneurysms in patients with history of KD. While the role of imaging in following patients with KD has been previously investigated, this is the first reported experience with the novel CR visualization methodology, and these examples demonstrate the potential of this technique for evaluating such complex vascular pathologic states.
Evaluation of Kawasaki’s disease-associated coronary artery aneurysms with 3D CT cinematic rendering
Rowe SP, Zimmerman SL, Johnson PT, Fishman EK
Emergency Radiology (2018) 25:449–453 - "Kawasaki’s disease (KD) is a vasculitis that predominantly affects children and can lead to the development of coronary artery aneurysms. These aneurysms can subsequently thrombose and occlude, which may lead to chest pain and other signs and symptoms of acute coronary syndrome in young patients. Coronary CT angiography, including 3D visualization techniques, is a common modality used in the follow-up of KD patients."
Evaluation of Kawasaki’s disease-associated coronary artery aneurysms with 3D CT cinematic rendering
Rowe SP, Zimmerman SL, Johnson PT, Fishman EK
Emergency Radiology (2018) 25:449–453 - "The most important potential complication of KD is in- flammatory damage to the coronary arteries, which classically leads to the formation of coronary artery aneurysms. These aneurysms will often undergo vascular remodeling and partial
thrombosis in order to produce a psuedonormal vascular lumen. However, progressive thrombosis and other stenotic processes such as fibrosis can, over time, precipitate cardiac ischemia that can lead to emergency room presentations for chest pain or other signs of acute coronary syndrome and necessitate invasive and/or surgical interventions."
Evaluation of Kawasaki’s disease-associated coronary artery aneurysms with 3D CT cinematic rendering
Rowe SP, Zimmerman SL, Johnson PT, Fishman EK
Emergency Radiology (2018) 25:449–453 - " While the advantages of this new technique are still under investigation, potential applications include improved visualization of complex anatomic structures that obviates the need for expensive 3D printing, better display of soft tissue texture that may improve detection and characterization of subtle lesions, improved pre-operative planning, and better trainee and patient engagement."
Evaluation of Kawasaki’s disease-associated coronary artery aneurysms with 3D CT cinematic rendering
Rowe SP, Zimmerman SL, Johnson PT, Fishman EK
Emergency Radiology (2018) 25:449–453 - "As with other 3D visualization methods, CR would be expected to provide a global overview of the disease process that is not easily appreciated on 2D axial or multi-planar reformatted images. In particular, this may help to identify relatively distal, small caliber sites of aneurysmal enlargement, which stand out with high contrast on the 3D images but can be subtle when only 2D images are viewed."
Evaluation of Kawasaki’s disease-associated coronary artery aneurysms with 3D CT cinematic rendering
Rowe SP, Zimmerman SL, Johnson PT, Fishman EK
Emergency Radiology (2018) 25:449–453 - "Given the anatomic complexity of the mediastinum with many adjacent vascular structures, it may be that CR has intrinsic advantages relative to other 3D methods in being able to accurately display the relative positions of those structures in a manner that may be more intuitively grasped in comparison to less photorealistic depictions. At the same time, the shadowing effects produced by CR can potentially obscure important sites of pathology, so a careful inspection of CR visualizations from multiple viewing angles and with multiple different window settings is necessary."
Evaluation of Kawasaki’s disease-associated coronary artery aneurysms with 3D CT cinematic rendering
Rowe SP, Zimmerman SL, Johnson PT, Fishman EK
Emergency Radiology (2018) 25:449–453
- “The majority of coronary arterial anomalies do not have clinical repercussions and do not need intervention. However, some anomalies can intermittently or chronically impede myocardial perfusion, leading to clinical manifestations such as angina, myocardial infarction, congestive heart failure, ventricular aneurysms, or sudden cardiac death.”
Anomalous Coronary Arteries That Need Intervention: Review of Pre- and Postoperative Imaging Appearances Agarwal PP et al. RadioGraphics 2017; 37:740–757 - “In a data analysis from a large U.S. national registry of competitive athletes, spanning a period of 27 years (1980–2006), anomalous coronary arteries were the second most common causeof SCD, accounting for 17% (119 of 1049) of SCDs, after hypertrophic cardiomyopathy, which accounted for 36%.”
Anomalous Coronary Arteries That Need Intervention: Review of Pre- and Postoperative Imaging Appearances Agarwal PP et al. RadioGraphics 2017; 37:740–757 - “The RCA and LCA fistulas most commonly drain into the right heart with common sites being the right ventricle, right atrium, pulmonary artery, and coronary sinus. Drainage into the left heart is rare, with drainage into the left atrium being slightly more common than into the left ventricle.”
Anomalous Coronary Arteries That Need Intervention: Review of Pre- and Postoperative Imaging Appearances Agarwal PP et al. RadioGraphics 2017; 37:740–757 - “CAFs are unlikely to close spontaneously (1%– 2% spontaneous closure rate) .Therefore, transcatheter or surgical closure may be considered in childhood even in asymptomatic patients, to avoid complications in adult life. Current recommendations include closure of large CAFs irrespective of symptoms, and treatment of small- to-medium stulas when the patients become symptomatic .”
Anomalous Coronary Arteries That Need Intervention: Review of Pre- and Postoperative Imaging Appearances Agarwal PP et al. RadioGraphics 2017; 37:740–757 - “Surgical options are usually reserved for cases where transcatheter treatment cannot be completed due to high-risk proximity to an adjacent coronary artery, multiple stulous
connections, or difficult access to the abnor- mal coronary artery or its branches. Surgery may also be preferred if there is a coexisting condition that warrants surgical management. Options include external ligation of the CAF, internal patch, or suture closure of the ori ce of the fistulous communication.”
Anomalous Coronary Arteries That Need Intervention: Review of Pre- and Postoperative Imaging Appearances Agarwal PP et al. RadioGraphics 2017; 37:740–757
- “The inclusion of CAC, in combination with clinical risk assessment, has high clinical value in patients with acute chest pain, as it identifies patients at low risk for ACS and obstructive CAD more accurately as com- pared to clinical risk assessment alone.”
Identification of coronary artery calcification can optimize risk stratification in patients with acute chest pain Bittner DO et al International Journal of Cardiology 249 (2017) 473–478 - “Whereas conventional risk factors can indicate the likelihood of CAD, coronary artery calcification (CAC) represents direct evidence of coronary atherosclerosis and thus can significantly improve 10-year CHD risk prediction in combination with traditional risk factors. As shown in asymptomatic patients, CAC scoring has been studied extensively and is well established by using non-contrast ECG-gated computed tomography of the heart. Although the negative predictive value (NPV) was consistently demonstrated to be high, in symptomatic patients the assessment of CAC does not play a major role, as obstructive CAD cannot be ruled out completely using non-contrast scans of the heart.”
Identification of coronary artery calcification can optimize risk stratification in patients with acute chest pain Bittner DO et al International Journal of Cardiology 249 (2017) 473–478
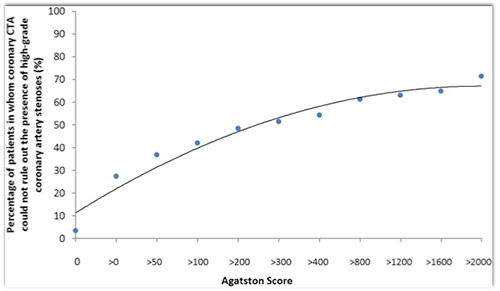
- BACKGROUND: Recent guidelines for the workup of patients with chest pain and suspected coronary artery disease include coronary computed tomography angiography (CTA). However, its diagnostic value may be limited in patients with severe coronary calcification.
CONCLUSION: In the largest patient series evaluated so far, we identified an "Agatston Score" of 287 to represent a threshold above which coronary CTA permits to rule out coronary artery stenoses in less than 50% of cases. Influence of the coronary calcium score on the ability to rule out coronary artery stenoses by coronary CT angiography in patients with suspected coronary artery disease. Schuhbaeck A et al J Cardiovasc Comput Tomogr. 2016 Sep-Oct;10(5):343-50 - “ The median coronary calcium score was 12, with calcium present in 60.5% of all patients. Coronary CTA ruled out stenoses in 82% of patients, while in 18% of patients at least one stenosis was found or could not be excluded. The threshold above which coronary CTA permitted to rule out stenoses in less than 50% of patients was an "Agatston Score" of 287. This threshold was significantly lower for male patients (213 vs. 330), for patients with a heart rate >65 beats/min (157 vs. 317) and for patients with a body mass index ≥25 kg/m(2) (208 vs. 392). The evaluability of coronary arteries decreased with increasing amounts of calcium and differed significantly between heart rates ≤65 beats/min and >65 beats/min (p < 0.0001).”
Influence of the coronary calcium score on the ability to rule out coronary artery stenoses by coronary CT angiography in patients with suspected coronary artery disease. Schuhbaeck A et al J Cardiovasc Comput Tomogr. 2016 Sep-Oct;10(5):343-50 - “The evaluability of coronary arteries decreased with increasing amounts of calcium and differed significantly between heart rates ≤65 beats/min and >65 beats/min (p < 0.0001).”
Influence of the coronary calcium score on the ability to rule out coronary artery stenoses by coronary CT angiography in patients with suspected coronary artery disease. Schuhbaeck A et al J Cardiovasc Comput Tomogr. 2016 Sep-Oct;10(5):343-50 - “The presence of pronounced coronary calcification has been identified as a limitation of coronary CTA, and in some guidelines, the use of coronary CTA is not encouraged for individuals above a certain amount of coronary calcium, e.g. an “Agatston Score” of 400.”
Influence of the coronary calcium score on the ability to rule out coronary artery stenoses by coronary CT angiography in patients with suspected coronary artery disease. Schuhbaeck A et al J Cardiovasc Comput Tomogr. 2016 Sep-Oct;10(5):343-50 - “First of all, with increasing amounts of coronary calcium, the prevalence of coronary stenoses increases making a “negative” coronary CTA unlikely and increasing the likelihood for the requirement of further downstream testing. Second, calcium might render coronary CTA data sets difficult to interpret or even unevaluable. Finally, extensive calcifications frequently cause overestimation of coronary stenosis severity, again leading to subsequent and potentially unnecessary testing.”
Influence of the coronary calcium score on the ability to rule out coronary artery stenoses by coronary CT angiography in patients with suspected coronary artery disease. Schuhbaeck A et al J Cardiovasc Comput Tomogr. 2016 Sep-Oct;10(5):343-50
- “We were able to demonstrate in a relative large cohort of 2614 patients with suspected coronary artery disease who were investigated by dual source computed tomography that this threshold was an “Agatston Score” of 287 for an overall all-comer patient group. In subgroup analyses with respect to gender, heart rate, body weight or body mass index, we found that the threshold can be substantially higher – both due to a lower prevalence of stenosis (e.g. in female patients) and due to a higher rate of fully evaluable data sets (e.g. in patients with low heart rate or low body weight, the former reducing motion artifacts and the latter leading to lower image noise.”
Influence of the coronary calcium score on the ability to rule out coronary artery stenoses by coronary CT angiography in patients with suspected coronary artery disease. Schuhbaeck A et al J Cardiovasc Comput Tomogr. 2016 Sep-Oct;10(5):343-50 - “Our study revealed that an “Agatston Score” > 287 represents a threshold above which coronary CTA, when performed with state-of-the-art technology and careful patient preparation, permits to rule out coronary stenoses in less than 50% of patients. However, there is substantial influence of other factors that determine image quality and hence that threshold, namely body weight or BMI (surrogate markers of image noise) as wells as heart rate (since motion aggravates artifacts caused by coronary calcium).”
Influence of the coronary calcium score on the ability to rule out coronary artery stenoses by coronary CT angiography in patients with suspected coronary artery disease. Schuhbaeck A et al J Cardiovasc Comput Tomogr. 2016 Sep-Oct;10(5):343-50 - “Despite of the limitations, the threshold identified in our study, an “Agatston Score” of 287, may be a useful value above which physicians performing coronary CTA may expect to be unable to rule out coronary artery stenoses in more than 50% of cases. If all imaging conditions are optimal, this threshold is 454.”
Influence of the coronary calcium score on the ability to rule out coronary artery stenoses by coronary CT angiography in patients with suspected coronary artery disease. Schuhbaeck A et al J Cardiovasc Comput Tomogr. 2016 Sep-Oct;10(5):343-50 - Calcium Score and CCTA
- “ First of all, with increasing amounts of coronary calcium, the prevalence of coronary stenoses increases making a “negative” coronary CTA unlikely and increasing the likelihood for the requirement of further downstream testing. Second, calcium might render coronary CTA data sets difficult to interpret or even unevaluable. Finally, extensive calcifications frequently cause overestimation of coronary stenosis severity, again leading to subsequent and potentially unnecessary testing.”
Influence of the coronary calcium score on the ability to rule out coronary artery stenoses by coronary CT angiography in patients with suspected coronary artery disease Annika Schuhbaeck et al. Journal of Cardiovascular Computed Tomography 10 (2016) 343-350 - “Despite of the limitations, the threshold identified in our study, an “Agatston Score” of 287, may be a useful value above which physicians performing coronary CTA may expect to be unable to rule out coronary artery stenoses in more than 50% of cases. If all imaging conditions are optimal, this threshold is 454. This may prompt preference of other clinical tests for patient evaluation.”
Influence of the coronary calcium score on the ability to rule out coronary artery stenoses by coronary CT angiography in patients with suspected coronary artery disease Annika Schuhbaeck et al. Journal of Cardiovascular Computed Tomography 10 (2016) 343-350 - “The median coronary calcium score was 12, with calcium present in 60.5% of all patients. Cor- onary CTA ruled out stenoses in 82% of patients, while in 18% of patients at least one stenosis was found or could not be excluded. The threshold above which coronary CTA permitted to rule out stenoses in less than 50% of patients was an “Agatston Score” of 287. This threshold was significantly lower for male patients (213 vs. 330), for patients with a heart rate >65 beats/min (157 vs. 317) and for patients with a body mass index !25 kg/m2 (208 vs. 392). The evaluability of coronary arteries decreased with increasing amounts of calcium and differed significantly between heart rates 65 beats/min and >65 beats/min (p < 0.0001).”
Influence of the coronary calcium score on the ability to rule out coronary artery stenoses by coronary CT angiography in patients with suspected coronary artery disease Annika Schuhbaeck et al. Journal of Cardiovascular Computed Tomography 10 (2016) 343-350 - “Cardiovascular risk assessment has assumed a prominent role in the course of preventive care of all adults. Traditionally cardiovascular risk assessment has been performed using risk factors including gender, age, smoking history, lipid status, diabetes status, and family history. Increasingly, imaging has been deployed to directly detect coronary atherosclerotic disease. Quantification of coronary calcium (e.g., Agatston method, calcium mass and volume) is readily detected using helical CT scanners. Large multicenter cohort studies have enabled a better understanding of the relevance of coronary calcium detection. The purpose of this review is to review the methods for quantification of coronary artery calcium, as well as to present current and future perspectives on calcium scoring for cardiovascular risk stratification.”
CT calcium scoring. History, current status and outlook. Sandfort V, Bluemke DA Diagn Interv Imaging. 2016 Aug 5. - Question: Diameters of coronary artery aneurysms (CAAs) complicating acute phase KD can strongly predict the long-term prognosis of coronary artery lesions (CAL). Recently, computed tomographic angiography (CTA) has been used to detect CAL, and the purpose of this study was to determine whether coronary artery diameters measurements by CTA using dual-source computed tomography (DSCT) can be used instead of coronary angiogram (CAG) measurements.
Measurements of Coronary Artery Aneurysms Due to Kawasaki Disease by Dual-Source Computed Tomography (DSCT) Tsujii N et al. Pediatr Cardiol. 2016 Mar;37(3):442-7. doi: 10.1007/s00246-015-1297-z. Epub 2015 Oct 29. - “Diagnostic accuracy was expressed as κ coefficient. A Bland-Altman analysis was also used to assess the intra-observer, inter-observer and inter-modality agreement. The diagnostic quality of CTA was excellent (κ = 0.93). Excellent inter-observer agreement for the diameters of CAAs was obtained for MIP, MPR and CAG and for the intra-observer agreement. The inter-modality agreement was also excellent in measurements of CAA (MPR-CAG: y = 0.9x + 0.40, r = 0.97, p < 0.0001 MIP-CAG: y = x + 0.1, r = 0.94, p < 0.0001). These values in normal coronary arteries were also obtained. We found a significant correlation between CTA and CAG in measuring the coronary arteries. We conclude that measuring coronary artery diameters by CTA is reliable and useful.”
Measurements of Coronary Artery Aneurysms Due to Kawasaki Disease by Dual-Source Computed Tomography (DSCT) Tsujii N et al. Pediatr Cardiol. 2016 Mar;37(3):442-7. doi: 10.1007/s00246-015-1297-z. Epub 2015 Oct 29. - “Excellent inter-observer agreement for the diameters of CAAs was obtained for MIP, MPR and CAG and for the intra-observer agreement. The inter-modality agreement was also excellent in measurements of CAA (MPR-CAG: y = 0.9x + 0.40, r = 0.97, p < 0.0001 MIP-CAG: y = x + 0.1, r = 0.94, p < 0.0001). These values in normal coronary arteries were also obtained. We found a significant correlation between CTA and CAG in measuring the coronary arteries. We conclude that measuring coronary artery diameters by CTA is reliable and useful.”
Measurements of Coronary Artery Aneurysms Due to Kawasaki Disease by Dual-Source Computed Tomography (DSCT) Tsujii N et al. Pediatr Cardiol. 2016 Mar;37(3):442-7.. - PURPOSE:“ Coronary-pulmonary arterial fistulas (CPAFs) are rare coronary artery anomalies that have been described only in limited case reports. This study aims to evaluate the clinical presentation and imaging findings of CPAFs collected from 6 participating medical centers along with CPAFs reported in the literature, to discern any general trends present in CPAFs.”
Coronary-Pulmonary Artery Fistulas: A Systematic Review. Verdini D et al. J Thorac Imaging. 2016 Nov;31(6):380-390. - CONCLUSIONS: “ CPAFs are seen in a variety of clinical settings, from infants with advanced congenital heart disease to elderly patients who have undergone revascularization surgery. Although coronary artery fistulas have previously been described as rarely involving multiple coronary arteries, with the right coronary artery being most often involved, our series demonstrates that multiple fistulas are commonly present, with the most common pattern being between the left main/left anterior descending and the main pulmonary trunk.”
Coronary-Pulmonary Artery Fistulas: A Systematic Review. Verdini D et al. J Thorac Imaging. 2016 Nov;31(6):380-390. - “Kawasaki disease (KD) is the most recognized vasculitis of childhood. The condition's characteristic high fever, rash, mucositis, conjunctivitis, lymphadenopathy, and extremity changes are superficially unexceptional, and resolve spontaneously within a mean of 12 days. It is the acuity and the potential for life-changing damage to the coronary arteries that distinguish KD from conditions that mimic it and exemplify the unique aspects and challenges of vascular inflammation in children.”
Kawasaki Disease at 50 Years. Cohen E, Sundel R JAMA Pediatr. 2016 Nov 1;170(11):1093-1099. - “Kawasaki disease is a hybrid condition at the junction of infectious diseases, immunology, rheumatology, and cardiology. Rather than being left an orphan disease, KD is bringing disciplines together to identify its genetic, pathophysiological, and hemodynamic features. In turn, this work promises to shed light on many other inflammatory conditions as well.”
Kawasaki Disease at 50 Years. Cohen E, Sundel R JAMA Pediatr. 2016 Nov 1;170(11):1093-1099. - “Inter-observer agreement between the study reviewers was moderate to good (0.4–0.73) for most of the incidental cardiovascular findings. At least one incidental cardiovascular finding not documented in the original report was identified by the study reviewers in 225/409 (55 %) of chest CT examinations. A total of 168/266 (63.2 %) potentially clinically significant cardiovascular findings were unreported in the original reports of 177/447 (39.6 %) subjects (p < 0.0001). Senior radiologists tended to more frequently report coronary artery calcification (p = 0.0006), cardiac valves calcification (p = 0.0003), and ascending aorta enlargement (p = 0.01) compared to junior radiologists.”
Under‐reporting of cardiovascular findings on chest CT Nicola Sverzellati et al. Radiol med (2016) 121:190–199 - “In keeping with our study, local radiologists only seldom specified which coronary artery was calcified. However, it was shown that visually scoring CAC on ungated CT is feasi- ble and of prognostic value. We could not stratify the prognostic value of CAC in our study cohort as the study observers applied a different CAC classification system.”
Under‐reporting of cardiovascular findings on chest CT Nicola Sverzellati et al. Radiol med (2016) 121:190–199 - “For both readers, there was no significant difference in agreement with the reference standard for per-vessel stenosis scores using either the 3D workstation or the iPad. In a multivariable logistic regression analysis including reader, workstation, and vessel as co-variates, there was no significant association between workstation type or reader and agreement with the reference standard (p > 0.05). Both readers identified 100 % of coronary anomalies using each technique.Reading of coronary CT angiography examinations on the iPad had no influence on stenosis assessment compared to the standard clinical workstation.”
Remote reading of coronary CTA exams using a tablet computer: utility for stenosis assessment and identification of coronary anomalies Stefan L. Zimmerman, Cheng T. Lin, Linda C. Chu, John Eng, Elliot K. Fishman Emerg Radiol (2016) 23:255–261


- “This multicenter ‘real world’ study demonstrates that use of advanced second generation dual-source CT scanners with high-pitch scanning capability results in significant radiation dose reduction in patients undergoing routine thoracic CT angiography without compromising diagnostic image quality. Reference levels for present generation scanners are pre- sented, but further confirmation from additional studies is required.”
CT dose reduction using prospectively triggered or fast-pitch spiral technique employed in cardiothoracic imaging (the CT dose study) Chinnaiyan KM et al. J Cardiovascular Comput Tomogr 8 (2014) 205-214 - “A significant dose difference was observed between high-pitch and non high-pitch modes at a median dose of 2.4 vs 5.1 mSv (P < .0001).”
CT dose reduction using prospectively triggered or fast-pitch spiral technique employed in cardiothoracic imaging (the CT dose study) Chinnaiyan KM et al. J Cardiovascular Comput Tomogr 8 (2014) 205-214 - Cardiac CTA: Developing a Practice
• Hours of availability
• Remote access for interpretation of study
• Training and retraining of Radiologists and Radiologic Technologists
• Interaction with referring physicians in the ER setting - “We need to move away from mandatory testing for every possible disease and move toward testing for serious conditions that the patient may have. We should, of course, do this with the minimal harm to patients. Providers should be able to, in most cases, decide whether they need to rule out coronary dis- ease, PE, or aortic dissection and select the test that will give them the best answer.”
Triple Rule Out CTA Scans or the Right Test for the Right Patient Hollander JE, Chang AM JACC: CARDIOVASCULAR IMAGING VOL. 8, NO. 7, 2015 pg 826-827 - “We know that coronary CTA and TRO CTA are similar with respect to the diagnosis of coronary disease. There is not enough evidence to determine whether TRO compares favorably or unfavorably with dedicated angiography of the pulmonary arteries or the aorta. Until we know that TRO CTA at least meets that bar, we probably should avoid the extra contrast and radiation that come along with it. Let’s use the right test for the right patient rather than a 1-test-fits-all approach.”
Triple Rule Out CTA Scans or the Right Test for the Right Patient Hollander JE, Chang AM JACC: CARDIOVASCULAR IMAGING VOL. 8, NO. 7, 2015 pg 826-827 - “Myocardial bridging is a congenital anomaly in which a segment of a coronary artery takes a "tunneled" intramuscular course under a "bridge" of overlying myocardium. This causes vessel compression in systole, resulting in hemodynamic changes that may be associated with angina, myocardial ischemia, acute coronary syndrome, left ventricular dysfunction, arrhythmias, and even sudden cardiac death.”
Myocardial Bridging: An Up-to-Date Review. Lee MS, Chen CH J Invasive Cardiol. 2015 Nov;27(11):521-8 - “Atherosclerosis preferentially develops immediately proximal to the bridged segment, likely due to alterations in shear stress, while the compressed segment itself is often spared. First-line therapy of symptomatic bridging remains medical treatment with beta-blockers and non-dihydropyridine calcium-channel blockers, and nitrates are contraindicated. Surgical myotomy, intracoronary stenting, and coronary artery bypass graft surgery have been used for refractory symptoms, but long-term outcomes remain uncertain.”
Myocardial Bridging: An Up-to-Date Review. Lee MS, Chen CH J Invasive Cardiol. 2015 Nov;27(11):521-8 - “Atherosclerosis preferentially develops immediately proximal to the bridged segment, likely due to alterations in shear stress, while the compressed segment itself is often spared.”
Myocardial Bridging: An Up-to-Date Review. Lee MS, Chen CH J Invasive Cardiol. 2015 Nov;27(11):521-8 - “Myocardial bridging, first described anatomically by Reyman in 1737, is a congenital variant of a coronary artery in which a portion of an epicardial coronary artery (most frequently the middle segment of the left anterior descending [LAD] artery) takes an intramuscular course. This arrangement of a “tunneled” segment of the artery under the “bridge” of overlying myocardium frequently results in vessel compression during systole. While frequently asymptomatic, this condition in many cases may be responsible for adverse complications including angina, myocardial ischemia, acute coronary syndromes, left ventricular dysfunction and stunning, arrhythmias, and even sudden cardiac death.”
Myocardial Bridging: An Up-to-Date Review. Lee MS, Chen CH J Invasive Cardiol. 2015 Nov;27(11):521-8 - “Myocardial bridging, first described anatomically by Reyman in 1737, is a congenital variant of a coronary artery in which a portion of an epicardial coronary artery (most frequently the middle segment of the left anterior descending [LAD] artery) takes an intramuscular course. This arrangement of a “tunneled” segment of the artery under the “bridge” of overlying myocardium frequently results in vessel compression during systole.”
Myocardial Bridging: An Up-to-Date Review. Lee MS, Chen CH J Invasive Cardiol. 2015 Nov;27(11):521-8 - “While frequently asymptomatic, this condition in many cases may be responsible for adverse complications including angina, myocardial ischemia, acute coronary syndromes, left ventricular dysfunction and stunning, arrhythmias, and even sudden cardiac death.”
Myocardial Bridging: An Up-to-Date Review. Lee MS, Chen CH J Invasive Cardiol. 2015 Nov;27(11):521-8 - “Myocardial bridging is a congenital anomaly in which an epicardial coronary artery takes an intramyocardial course. It is present anatomically in approximately 25% of patients based on autopsy and CT, but only results in angiographically detectable systolic compression in less than 10% of patients.”
Myocardial Bridging: An Up-to-Date Review. Lee MS, Chen CH J Invasive Cardiol. 2015 Nov;27(11):521-8 - “Mechanisms of acute myocardial infarction and nonobstructed coronary arteries (MINOCA) are incompletely understood. Myocardial bridging (MB) is usually considered a benign congenital variant, but serious complications have been reported. MB has also been proposed as a cause of takotsubo syndrome (TS). We aimed to examine whether MB was more frequent in patients with MINOCA or TS than in age- and gender-matched controls and to compare the MB detection rates of coronary computed tomography angiography (CTA) and invasive coronary angiography (ICA).”
Prevalence of Myocardial Bridging in Patients With Myocardial Infarction and Nonobstructed Coronary Arteries Brolin EB et al. Am J Cardiol. 2015 Oct 3. [Epub ahead of print] - “There were no statistically significant differences regarding the prevalence of MB or the type, location, length, or thickness of MB. There was a statistically significant difference (p <0.01) between the detection rates of coronary CTA and ICA that demonstrated MB in 54 subjects (47%) and 13 subjects (23%), respectively. In conclusion, MB was frequent with a similar prevalence in patients with MINOCA, patients with TS and controls. This suggests that there is no causal link between MB and MINOCA or TS. Furthermore, coronary CTA detects MB at a significantly higher rate than ICA..”
Prevalence of Myocardial Bridging in Patients With Myocardial Infarction and Nonobstructed Coronary Arteries Brolin EB et al. Am J Cardiol. 2015 Oct 3. [Epub ahead of print] - “In conclusion, MB was frequent with a similar prevalence in patients with MINOCA, patients with TS and controls. This suggests that there is no causal link between MB and MINOCA or TS. Furthermore, coronary CTA detects MB at a significantly higher rate than ICA.”
Prevalence of Myocardial Bridging in Patients With Myocardial Infarction and Nonobstructed Coronary Arteries Brolin EB et al. Am J Cardiol. 2015 Oct 3. [Epub ahead of print] - “Myocardial bridging of coronary arteries is common on CTA, but only approximately one-third of these show systolic compression. Myocardial bridging is not associated with reduced myocardial perfusion during vasodilator stress. Atherosclerosis is located predominantly proximal to myocardial bridging but atherosclerotic burden and presence of vulnerable plaques were comparable.”
The Functional Effects of Intramural Course of Coronary Arteries and its Relation to Coronary Atherosclerosis. Uusitalo V et al. JACC Cardiovasc Imaging. 2015 Jun;8(6):697-704 - Takotsubo Syndrome
• Takotsubo syndrome is an acute reversible heart failure syndrome that is increasingly recognized in modern cardiology practice.
• Takotsubo syndrome (TS), also known as stress-induced cardiomyopathy, is an acute cardiac syndrome associated with significant mortality and morbidity. It is found in approximately 2–5% of patients presenting with acute coronary syndromes (ACS). TS patients typically receive ACS therapy, the consequences of which are largely unknown but may lead to unnecessary complications. - Takotsubo Syndrome (2012, Johns Hopkins criteria)
Mandatory criteria
• Absence of coronary thrombosis or angiographic evidence of acute plaque rupture
• Regional ventricular wall motion abnormalities that extend beyond a single epicardial vascular distribution
• Complete recovery of reginal wall motion abnormalities (usually within days to weeks) - Takotsubo Syndrome (2012, Johns Hopkins criteria)
Helpful, but not mandatory, criteria
• An acute identifiable trigger (either emotional or physical)
• Characteristic ECG changes that may include some or all of the following:
• – ST-segment elevation at time of admission (often ≤2 mm in magnitude, and usually not associated with reciprocal ST-segment depression)
• – Diffuse deep T-wave inversion (may be present on admission or may evolve during the first several hospital days)
• – QT interval prolongation (usually maximal by 24–48 h)
• Mildly elevated cardiac troponin
• (often appears disproportionately low given the degree of wall motion abnormality) - “Broken heart syndrome is a temporary heart condition that's often brought on by stressful situations, such as the death of a loved one. People with broken heart syndrome may have sudden chest pain or think they're having a heart attack. In broken heart syndrome, there's a temporary disruption of your heart's normal pumping function, while the remainder of the heart functions normally or with even more forceful contractions. Broken heart syndrome may be caused by the heart's reaction to a surge of stress hormones. The condition may also be called takotsubo cardiomyopathy, apical ballooning syndrome or stress cardiomyopathy by doctors.The symptoms of broken heart syndrome are treatable, and the condition usually reverses itself in about a week.”
Mayo Clinic Newsletter March 2014
- “Because of the complexity of coronary anatomy, the frequency of motion and calcium-related image artifacts, and the morphologic subtleties of lesions,
interpreters must review coronary CTA interactively on cardiac-specific interpretation software platforms capable of 2- and 3-dimensional displays in all conventional reconstruction formats. These include transaxial 2-dimensional image stacks, multiplanar reformations (MPR), maximum intensity projections (MIP), curved multiplanar reformations (cMPR), and volume rendering technique (VRT) reconstructions.”
SCCT guidelines for the interpretation and reporting of coronary CT angiography: A report of the Society of Cardiovascular Computed Tomography Guidelines Committee Leipsic et al. J Cardiovasc Comput Tomogr. 2014;8:342-358 - Reconstruction of CCTA Data
• Axial
• Multiplanar reconstruction
• Curved planar reconstruction
• Maximum intensity projection (MIP)
• Volume rendering technique - “Description of plaques as “noncalcific” is preferable to “soft” or “lipid rich” as low CT density (HU) levels do not necessarily correlate closely with anatomic pathology or biochemistry. It is recommended that features of plaque morphology such as ulceration, dissection, and fissuring be noted when image quality is sufficient.”
SCCT guidelines for the interpretation and reporting of coronary CT angiography: A report of the Society of Cardiovascular Computed Tomography Guidelines Committee Leipsic et al. J Cardiovasc Comput Tomogr. 2014;8:342-358 
- Cardiac CT Stenosis Grading
• 0-Normal: absence of plaque and no luminal stenosis
• 1-Minimal: plaque with <25% stenosis
• 2-Mild: 25% to 49% stenosis
• 3-Moderate: 50% to 69% stenosis
• 4-Severe: 70% to 99% stenosis
• 5-Occluded - Extracardiac Structures
• Lung parenchyma
• Mediastinum
• Pleural surface
• Esophagus
• Chest wall
• Upper abdomen (including liver) - Cardiac CTA Report Components
• Study indication
• Clinical data
• Study protocol (injection rate etc.)
• Results
• Scan quality
• Clinical scan findings
• Impression - “Documentation of the date of electronic or physical signature should be included in the report. It is recommended that all potentially life-threatening findings are reported to the referring physician on the same date of the study and that a record of a verbal communication be included in the report. Reports of emergency studies should be issued within 24 hours, and elective studies should be reported within 2 working days of the procedure.”
SCCT guidelines for the interpretation and reporting of coronary CT angiography: A report of the Society of Cardiovascular Computed Tomography Guidelines Committee Leipsic et al. J Cardiovasc Comput Tomogr. 2014;8:342-358

- “Kawasaki disease (KD) is the leading cause of acquired coronary disease in children and may lead to subsequent myocardial ischemia and infarction. Because coronary computed tomographic angiography (CTA) is the most sensitive noninvasive test in patients with atherosclerosis, the aim of this study was to retrospectively evaluate coronary CTA performed in patients with KD for aneurysm, stenosis, and calcified and noncalcified coronary artery disease (CAD).”
Coronary Computed Tomographic Angiographic Findings in Patients With Kawasaki Disease.
Han BK,
Am J Cardiol. 2014 Sep 16. pii: S0002-9149(14)01776-7 - “In conclusion, high-risk patients with histories of KD had nonobstructive and obstructive CAD not visualized by other noninvasive imaging tests. In properly selected high-risk patients with KD, coronary CTA may identify a subset at increased risk for future coronary pathology who may benefit from medical therapy.”
Coronary Computed Tomographic Angiographic Findings in Patients With Kawasaki Disease.
Han BK,
Am J Cardiol. 2014 Sep 16. pii: S0002-9149(14)01776-7 - “Typical KD findings in both adults and children include fever, conjunctivitis, pharyngitis, skin erythema progressing to a desquamating rash on the palms and soles, and strawberry tongue. Adults more frequently present with cervical adenopathy (93% of adults versus 15% of children), hepatitis (65% versus 10%), and arthralgia (61% versus 24% to 38%). In contrast, adults are less frequently affected by meningitis (10% versus 34%), thrombocytosis (55% versus 100%), and coronary artery aneurysms (5% versus 18%– 25%).”
Coronary Artery Aneurysms After Adult-Onset Kawasaki Disease
Inokuchi R et al.
Circulation. 2013;127:1636-1637 - “KD is a common vasculitis of childhood, but adult-onset KD is rare. No specific diagnostic tests are available for KD; the diagnosis is based on the presence of characteristic clinical findings. In addition, a consensus does not exist regarding the treatment of adult-onset KD. The treatment of KD with high-dose intravenous immunoglobulin within the first 10 days of illness reportedly decreases the prevalence of coronary artery aneurysms in childhood.”
Coronary Artery Aneurysms After Adult-Onset Kawasaki Disease
Inokuchi R et al.
Circulation. 2013;127:1636-1637 - “As an alternative diagnostic modality, prospective ECG-triggered DSCTCA with excellent image quality and low radiation exposure has been proved useful for diagnosing infants and children with coronary artery aneurysms due to Kawasaki disease.”
Application of prospective ECG-triggered dual-source CT coronary angiography for infants and children with coronary artery aneurysms due to Kawasaki disease.
Duan Y et al.
Br J Radiol. 2012 Dec;85(1020):e1190-7 - “Kawasaki disease (KD), also known as mucocutaneous lymph node syndrome, is an autoimmune vasculitis in which the small and medium vessels throughout the body become inflamed. It predominantly occurs in infants and children (younger than 5 years old). It affects many organ systems; injury, such as aneurysm, dilation, ectasia, stenosis and embolism, to the heart is rare but serious, and fatal myocardial infarction can be induced in untreated cases . It is crucial to detect coronary artery lesions at an early stage. Diagnosis of KD is based on clinical signs, symptoms and laboratory findings, but no specific laboratory test exists and it is hard to establish the diagnosis, especially in the early course.”
Application of prospective ECG-triggered dual-source CT coronary angiography for infants and children with coronary artery aneurysms due to Kawasaki disease.
Duan Y et al.
Br J Radiol. 2012 Dec;85(1020):e1190-7
- Congenital Coronary Artery Anomalies: Classification
- Anomalies of aortic origin
- Anomalies of non-aortic origin
- Anomalies of course
- Anomalies of termination
- Anomalies of intrinsic coronary anatomy - Ectopic Origin from the Ascending Aorta: facts
- The LCA and/or the RCA originate from the ascending aorta above the sinotubular junction instead of the sinus of Valsalva
- The ectopic origin from ascending aorta is defined as a coronary artery arising 1 cm above the sinotubular junction
“ A broad spectrum of congenital coronary anomalies may be discovered on imaging and sometimes in the emergency setting on computed tomography (CT). Most coronary artery anomalies are of academic interest, however, a minority can cause morbidity and mortality and symptoms such as angina, myocardial infarction, or arrhythmias.”
Coronary anomalies encountered in the acute setting: am imaging review
Shuaib W et al.
Emerg Radiol (2014) 21:631-641 - Acute Chest Pain in the ER: Facts
- More tha 9 million ER visits each year in the US
- Related health care costs are in the 13-15 billion dollar range
- Incidence of cardiac event in patients with normal EKG and cardiac biomarkers (troponins) is 1-8% - Recommended Stenosis Grading for CCTA
- 0- normal: absence of plaque or no luminal stenosis
- 1- minimal: plaque with <25% stenosis
- 2- mild: 25%-49% stenosis
- 3- moderate: 50%-69% stenosis
- 4- severe: 70-99% stenosis
- 5- occluded - Sample management recommendations to ER Physicians
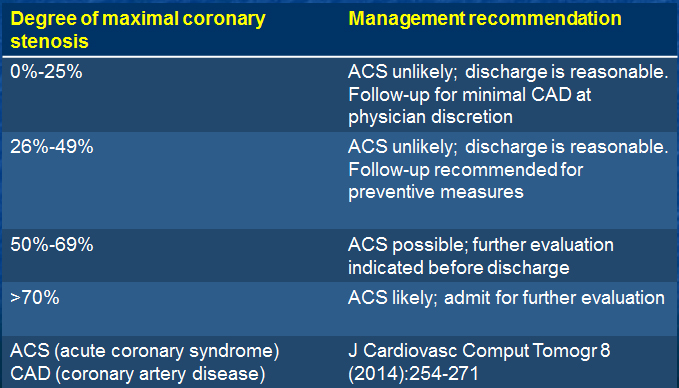
- “The Society of Cardiovascular Computed Tomography Guidelines Committee was formed to develop recommendations for acquiring, interpreting, and reporting of cardiovascular CT to ensure adequate, safe, and efficient use of this modality.”
SCCT guidelines on the use of coronary computed tomographic angiography for patients presenting with acute chest pain for the emergency department: A Report of the Society of Cardiovascular Computed Tomography Guideline Committee
Raff GL et al
J Cardiovasc Comput Tomogr 8 (2014):254-271
- “ In patients with Takayasu Arteritis, there is a high prevalence of coronary arterial abnormalities at coronary CT angiography, regardless of disease activity or symptoms. Thus coronary CT angiography may add information on coronary artery lesions in patients with Takayasu Arteritis.”
Takayasu Arteritis: Assessment of Coronary Arterial Abnormalities with 128-Section Dual-Source CT Angiography of the Coronary Arteries and Aorta
Kang EJ et al.
Radiology 2014;270:74-81 - “ More than half of patients with Takayasu Arteritis have coronary arterial lesions (stenosis or aneurysm) at coronary CT angiography, regardless of symptoms and disease activity.”
Takayasu Arteritis: Assessment of Coronary Arterial Abnormalities with 128-Section Dual-Source CT Angiography of the Coronary Arteries and Aorta
Kang EJ et al.
Radiology 2014;270:74-81
- Right coronary artery: Facts
- Arises from the right sinus
- Runs in the right AV groove toward the inferior interventicular septum
- Supplies blood to the sinoatrial node (60%), right atrium and ventricles
Branches:
- conus (first branch in 60%)
- SA nodal artery
- Atrial branches and RV branches
- Acute marginal branch (largest RV branch)
- PDA (70%) - Left main coronary artery: Facts
- Arises from the left sinus
- Variable in length or absent (<1%)
- Gives rise to LAD and circumflex. In 15% of patients also gives rise to ramus branch (trifurcation) - Left anterior descending coronary artery: Facts
- Arises from the left main
- Courses inferiorly in the anterior interventricular groove
Gives rise to diagonal branches
- Numbered D1 – Dx
- Highly variable in size and number
- Supply the anterior wall of the LV
Gives rise to septal perforators
- Supply the anterior 2/3 of the interventricular septum
- May wrap around apex to supply apical inferior wall/septum - Circumflex coronary artery
- Arises from the left main coronary artery
- Courses inferiorly in the left atrioventricular groove
Gives rise to obtuse marginal branches numbered OM1 – OMx
- Variable in size and number
- Supply lateral wall of the LV
- Gives rise to sinoatrial node in 40%
- Gives rise to PDA (dominant) in 10% - Anomalous termination:
Coronary fistulae
- Incidence of 0.1% during diagnostic cath
- RCA (55%) > LCA (35%) > both/other (10%)
- Majority congenital with a small number of iatrogenic cases
- Left to right shunt
- Coronary – pulmonary artery or coronary sinus can be seen
- Coronary – ventricle also occurs (coronary-cameral fistula)
- “The sinoatrial (SA) node artery was most frequently a large atrial branch of the right coronary artery (63%), arising at a mean distance of 1.2 cm (range 0.2 - 2.2 cm) from its beginning, with a mean external diameter of 1.7 mm (range 1 - 3 mm). In 37% of cases the SA node artery was a branch of the left coronary artery or one of its branches, with an initial mean external diameter of 2.2 mm (range 2 - 3 mm).”
Anatomical aspects of the arterial blood supply to the sinoatrial and atrioventricular nodes of the human heart
Pejkovic B et al.
J Int Med Res 2008 Jul-Aug:36(4):691-8
- Nonatherosclerotic Causes of Coronary Disease Seen on CCTA
- Anomalous coronary artery
- Coronary artery vasculitis
----Takayasu arteritis
----Kawasaki disease
- Coronary Embolism
- Infection
- Cardiac tumors with invasion
- Coronary artery spasm
- Coronary artery dissection - “ Cardiac MDCT can show various causes of nonatherosclerotic CADs and of coronary atherosclerosis. Radiologists should be aware of the diverse imaging findings of nonatherosclerotic, nonanomalous CADs that can be identified with cardiac MDCT to facilitate accurate diagnosis and proper management.”
Less Common Causes of Disease Involving the Coronary Arteries: MDCT Findings
Kim JA et al.
AJR 2011; 197:125-130 - “ Coronary calcium scoring (CCS) is useful for assessing coronary artery atherosclerosis. Our study assesses its role in this setting as alternative to stress-ECG. Adoption of CCS as an alternative to sECG could prove cost effective.”
Economic analysis of the use of coronary calcium scoring as an alternative to stress ECG in the non-invasive diagnosis of coronary artery disease
Raman V et al.
Eur Radiol 2011 Oct 13 (epub ahead of print) - "The transeptal, prepulmonic, and retroaortic courses are considered benign or clinically insignificant, and also referred to as nonmaligant anomalies, while an interarterial course is considered clinically significant, is also referred to as malignant anomaly, is potentially lethal, and can lead to sudden death in young adults."
Imaging of Coronary Artery Anomalies
Sundaram B et al.
Radiol Clin N Am 48 (2010)711-727 - Left Main Coronary Artery arises off the Right Coronary Artery: Pathways
- Course between the aorta and pulmonary artery at the level of pulmonary valve or right ventricular outflow (interarterial course)
- Transverse the upper intraventricular septum (transeptal course)
- Course anterior to the pulmonary artery or right ventricular outflow tract (prepulmonic course)
- Course between the aortic root and left atrium (retroaortic course) "The left main coronary artery (LMA) arises from the sinus of Valsalva (RSV), RCA or as a common trunk with the RCA in 0.10% of patients and in 75% of these patients the LMA has an interarterial course."
Imaging of Coronary Artery Anomalies
Sundaram B et al.
Radiol Clin N Am 48 (2010)711-727"Coronary artery aneurysms are uncommon lesions, with an overall incidence of 1.6%; incidence among individuals imaged with angiography is as high as 5%. Most commonly, these aneurysms involve the right coronary artery, followed by the left anterior descending coronary artery or left circumflex coronary artery."
CT Angiography of Coronary Artery Aneurysms: Detection, Definition, Causes and Treatment
Johnson PT, Fishman EK
AJR 2010; 195:928-934"Cardiac 64-slice MDCT provides excellent visualization of the origin, course, and distal vessel entry site of CCAF and the site of fistula entry."
Evaluation of Efficacy of 64-Slice Multidetector Computed Tomography in Patients With Congenital Coronary Fistulas
Dodd JD et al.
J Comput Assist Tomogr 2008; 32:265-270- Coronary Artery Fistulae: Facts
- Originate from the right coronary artery in two thirds of patients, the left coronary system in 25% and from both systems in 5%
- More than 90% of CCAF drain into the right atrium, coronary sinmus or right ventricle - Coronary Artery Fistulae: Facts
- Abnormal communication between a coronary artery and another vascular structure (artery, vein or cardiac chamber)
- Most common drainage is to right ventricle (45%), right atrium (25%) and the pulmonary artery (15%).
- Drainage can be to coronary sinus, SVC, as well as left atrium and ventricle "Cardiac 64-slice MDCT provides excellent visualization of the origin, course, and distal vessel entry site of CCAF and the site of fistula entry."
Evaluation of Efficacy of 64-Slice Multidetector Computed Tomography in Patients With Congenital Coronary Fistulas
Dodd JD et al.
J Comput Assist Tomogr 2008; 32:265-270- Coronary Artery Fistulae: Facts
- Originate from the right coronary artery in two thirds of patients, the left coronary system in 25% and from both systems in 5%
- More than 90% of CCAF drain into the right atrium, coronary sinmus or right ventricle - Coronary Artery Fistulae: Facts
- Abnormal communication between a coronary artery and another vascular structure (artery, vein or cardiac chamber)
- Most common drainage is to right ventricle (45%), right atrium (25%) and the pulmonary artery (15%).
- Drainage can be to coronary sinus, SVC, as well as left atrium and ventricle - Cardiac Anatomy : RCA
- In 50-60% of patients the first branch off the RCA is the conus artery
- In 30-35% of patients the conus artery arises directly from the aorta
- In approximately 58% of patients the sinoatrial nodal artery arises from the RCA
- In approximately 42% of patients the sinoatrial nodal artery arises from the left circumflex artery "Volume rendered images acquired from three dimensional CT data sets provides an excellent overview of the cardiac and vascular anatomy and helps surgeons understand the anatomic complexity before surgery."
Coronary Artery Fistulas:CT Findings
Zenooz et al.
RadioGraphics 2009;29:781-789- Coronary Artery Fistulae: Clinical Presentations
- Usually present as left to right shunt
- Continuous heart murmur common
- Symptoms include dyspnea, fatigue,chest pain, arrthymias, stroke, and myocardial ischemia/infarction
- Patients can present with sudden death - Coronary Artery Fistulae: Some Facts
- Arise from the RCA in approximately 50% of cases, the left coronary artery in 42% of patients and both the RCA and LCA in about 5% of cases
- Most symptomatic coronary artery fistulae arise from the RCA
- Most common drainage sites are right ventricle (41%) and right atrium (26%) - Coronary Artery Anomalies: Types Include
- Coronary artery fistulae is an anomaly of termination
- Coronary artery fistulae is a direct precapillary connection between a branch of the coronary artery and the lumen of a cardiac chamber, the coronary sinus, SVC, or pulmonary artery or vein close to heart "Therefore, in addition to evaluation of the coronary arteries for stenosis and plaques, special attention should be paid to their courses and terminations in every CT study of the heart to detect these potentially fatal anomalies."
Coronary Artery Fistulas:CT Findings
Zenooz et al.
RadioGraphics 2009;29:781-789- Coronary Artery Anomalies: Types Include
- Abnormalities of number
- Abnormalities of course
- Abnormalities of termination
- Abnormalities of structure - Coronary Artery Anomalies: Facts
- Are seen in 0.3%-1.3% of patients undergoing catheter angiography
- Are seen in 1% of routine autopsies
- Are seen in 4-15% of young individuals who experience sudden death - Coronary Artery Fistulas: Treatment
- Surgical ligation in patients with symptoms of myocardial ischemia, large right to left shunts, and congestive heart failure
- Coronary artery stents and coiling - Coronary Artery Fistulas: Definition
"Coronary artery fistulas, defined as abnormal vascular communications between any coronary artery and any of the cardiac chambers or great vessels"
MDCT of Left Anterior Descending Coronary Artery to Main Pulmonary Artery Fistula
Chang DS et al.
AJR 2005; 185:1258-1260 - Coronary Artery Fistulas: Presentation
- Incidental finding on coronary angiography or autopsy. The incidence in one series of adults undergoing coronary angiography was 0.18%
- Patients may be symptomatic and present with congestive heart failure, cardiomyopathy, myocardial ischemia or atrial fibrillation
- Most coronary artery fistulas drain into the right ventricle or pulmonary artery - Coronary Artery Fistulas: Etiology
- Congenital (most common)
- Complication of chest trauma
- Complication of coronary angioplasty
- Complication of coronary artery bypass surgery especially when internal mammary artery is used
- Complication of cardiac transplantation "It is important for CT interpreters to be aware of and recognize dual LAD at coronary CT. Because of inability to visualize the additional vessel, especially when the long LAD originates fro the right coronary sinus, the variant anatomic features can be misinterpreted at routine coronary angiography for mid-LAD occlusion"
Dual Left Anterior Descending Coronary Artery: CT Findings
Agarwal PP, Kazerooni EA
AJR 2008; 191:1698-1701- Classification of Dual LADs
type
Short course of LAD
Long course of LAD
I Origin from LAD proper, terminates high in ant. intervent groove (AIG)
Origin from LAD proper, descends on left ventricular side of AIG, and reenters distal AIG
II Origin from LAD proper, terminates high in ant. intervent groove (AIG)
Origin from LAD proper, descends on right ventricular side of AIG, and reenters distal AIG
III Origin from LAD proper, terminates high in ant. intervent groove (AIG)
Origin from LAD proper, intramyocardial in septum proximally and emerges in apical AIG or does not emerge and end with septal branches to apical septum
IV Origin from LAD proper, terminates high in ant. intervent groove (AIG)
Origin from right coronary artery, anomalous prepulmonic course and reenters AIG
- Dual Left Anterior Descending Coronary Artery: Facts
- 4 variants with differentiation based on both short course of LAD and long course of LAD
- Majority of cases has both vessels arising from LAD (types I,II,III) while occassionally the long course of the LAD arises from the RCA - Coronary Artery Aneurysms: Complications
- Thrombosis
- Embolic phenomenon
- Arteriovenous fistulization
- Spasm
- Rupture
- Hemopericardium (ominous sign of rupture or pending rupture) "With the increasing use of coronary CTA, radiologists must be cognizant of predisposing conditions and diagnostic criteria for coronary artery aneurysm to swiftly guide management and avert complications."
CT Angiography of Coronary Artery Aneurysms: Detection, Definition, Causes, and Treatment
Johnson PT, Fishman EK
AJR 2010; 195:928-934"Coronary artery aneurysms are uncommon lesions, with an overall incidence of 1.6%; incidence among individuals imaged with angiography is as high as 5%."
CT Angiography of Coronary Artery Aneurysms: Detection, Definition, Causes, and Treatment
Johnson PT, Fishman EK
AJR 2010; 195:928-934"Segmental agreement for stenoses 50% or greater and 70% or greater was greater than 96%. Disagreements were more likely in the presence of noneccentric calcification for both intraobserver and interobserver measurements."
64-Channel Cardiac Computed Tomography: Intraobserver and Interobserver Variability (part 1): Coronary Angiography
Nicol ED et al
J Comput Assist Tomogr 2009;33: 161-168- "Interobservor and intraobserver variability for the detection of coronary stenoses on CTA is good and justifies routine clinical use. The presence of noneccentric calcium and mixed plaque morphology are important causes of disagreement."
64-Channel Cardiac Computed Tomography: Intraobserver and Interobserver Variability (part 1): Coronary Angiography
Nicol ED et al
J Comput Assist Tomogr 2009;33: 161-168 - "We found that the incidence of myocardial bridging in asymptomatic adults is 7%, which is in agreement with some pathologic studies in the literature.Our study shows that MDCT of the coronary arteries is a reliable and noninvasive technique, ehich can accurately locate the site of myocardial bridging and measure its thickness, course and length."
Prevalence of myocardial bridging detected with 64-slice multidetector coronary computed tomography angiography in asymptomatic adults
Atar E et al.
J Cardiovasc Comput Tomogr (2007) 1, 78-83 - Myocardial Bridging: Definition
Myocardial bridging, first described by Reyman in 1737 is a congenital condition in which a segment of an epicardial artery has an intramural course within the myocardium. It is typically confined to a single vessel, usually the mid left anterior descending (LAD) artery.
- "Manual stenosis measurements are significantly more accurate compared with automatic measurements, and therefore, manual adjustments are still essential for noninvasive assessment of coronary artery stenosis." Accuracy of Noninvasive Coronary Stenosis Quantification of Different Commercially Available Dedicated Software Packages
Dikkers R et al.
J Comput Assist Tomogr 2009;33: 505-512 - "Purpose: the purpose of this study was to investigate the noninvasive quantification of coronary artery stenosis using cardiac software packages and vessel phantoms with known stenosis severity." Accuracy of Noninvasive Coronary Stenosis Quantification of Different Commercially Available Dedicated Software Packages
Dikkers R et al.
J Comput Assist Tomogr 2009;33: 505-512 - "Despite the high diagnostic accuracy of multidetector coronary computed tomographic angiography (CCTA) for the detection and exclusion of obstructive coronary artery stenosis, several technical limitations of current generation CT scanners may cause artifacts that prevent interpretation of images or cause misclassifications of lesions."
What makes a coronary CT angiogram nondiagnostic?
Min JK, Lin FY
J Cardiovasc Comput Tomogr (2008) 2, 351-359 - What is arterial dominance?
- The question is what artery is feeding the posterior interventricular septum
- It is the RCA in 67% of the population giving rise to the right posterior coronary artery and posterior lateral coronary artery
- It is the circumflex in 15% of the population giving rise to the left posterior coronary artery and left posterior lateral coronary artery
- Co-dominance occurs in 18% of patients - "Our study indicated that, although right dominance circulation is more common in the general population, both the coronary diseases and coronary artery variations are more common in individuals with left dominance circulation."
An Investigation of the Association Between Coronary Artery Dominance and Coronary Artery Variations with Coronary Arterial Disease by Multidetector Computed Tomographic Coronary Angiography
Eren S et al.
J Comput Assist Tomogr 2008;32:929-933 - "Volume rendered images acquired from three dimensional CT data sets provides an excellent overview of the cardiac and vascular anatomy and helps surgeons understand the anatomic complexity before surgery."
Coronary Artery Fistulas:CT Findings
Zenooz et al.
RadioGraphics 2009;29:781-789 - Coronary Artery Fistulae: Clinical Presentations
- Usually present as left to right shunt
- Continuous heart murmur common
- Symptoms include dyspnea, fatigue,chest pain, arrthymias, stroke, and myocardial ischemia/infarction
- Patients can present with sudden death - Coronary Artery Fistulae: Some Facts
- Arise from the RCA in approximately 50% of cases, the left coronary artery in 42% of patients and both the RCA and LCA in about 5% of cases
- Most symptomatic coronary artery fistulae arise from the RCA
- Most common drainage sites are right ventricle (41%) and right atrium (26%) - Coronary Artery Anomalies: Types Include
- Coronary artery fistulae is an anomaly of termination
- Coronary artery fistulae is a direct precapillary connection between a branch of the coronary artery and the lumen of a cardiac chamber, the coronary sinus, SVC, or pulmonary artery or vein close to heart - "Therefore, in addition to evaluation of the coronary arteries for stenosis and plaques, special attention should be paid to their courses and terminations in every CT study of the heart to detect these potentially fatal anomalies."
Coronary Artery Fistulas:CT Findings
Zenooz et al.
RadioGraphics 2009;29:781-789 - Coronary Artery Anomalies: Types Include
- Abnormalities of number
- Abnormalities of course
- Abnormalities of termination
- Abnormalities of structure - Coronary Artery Anomalies: Facts
- Are seen in 0.3%-1.3% of patients undergoing catheter angiography
- Are seen in 1% of routine autopsies
- Are seen in 4-15% of young individuals who experience sudden death - Dilated Cardiomyopathy: Causes
- Idiopathic causes
- Familial causes (20-35%)
- Various insults (drugs such as alcohol, anthracyclines, and catecholamines)
- Infection (viral, bacterial, fungal)
- Neuromuscular syndromes (Duchene musculsr dystrophy, Friedrich ataxia)
- Sudden Cardiac Death: Causes
- Coronary artery disease (75-80%)
- Myocarditis (5%)
- Dilated and infiltrative cardiomyopathies (10-15%)
- Sudden Cardiac Death: Causes
- Coronary artery disease (most common)
- Myocarditis
- Cardiac sarcoidosis
- Dilated and infiltrative cardiomyopathies
- Sources of CTA error in Gouya H et al. article
- Under or overestimation of the degree of stenosis
- Nonassessable coronary artery segments at MDCT caused by poor image quality
- Discordance between MDCT and coronary angiography in defining the coronary segments according to the American Heart Association classification. - "Despite excellent sensitivity and negative likelihood ratios in a per patient and per vessel analysis, some coronary artery stenosis remained misdiagnosed with 64-section CT, resulting in limited sensitivity on a per-segment basis owing to anatomic discordance and failure to accurately quantify intermediate stenosis."
Coronary Artery Stenosis in High-risk Patients:64-Section CT and Coronary Angiography-Prospective Study and Analysis of Discordance
Gouya H et al.
Radiology 2009; 252:377-385 - " This article formulates a practical approach for salvaging difficult or potentially uninterpretable studies by diagnosing the causes of artifacts and providing an approach for scan improvement with the reconstruction of new data sets."
Practical approaches to overcoming artifacts in coronary CT Angiography
Lesser JR et al.
J Cardiovasc Comout Tomogr (2009) 3, 4-15 - "ALCAPA syndrome is a rare congenital anomaly in which the LCA originates from the main pulmonary artery. The diagnosis can be made with ECG-gated multidetector CT angiography and MR imaging." ALCAPA Syndrome:Not Just a Pediatric Disease
Pena E et al.
Radiographics 2009; 29:553-565 - Dilatation of the Coronary Arteries: Causes
- Kawasaki disease
- Coronary artery-coronary sinus fistula
- Atherosclerosis related coronary artery ectasia
- Vasculitis (polyartritis nodosa or Takayasu arteritis)
- Ehlers Danlos syndrome
- Scleroderma
- Trauma - Isolated origin of the LAD, RCA or circumfles artery off the pulmonary artery can occur
- ALCAPA Syndrome
- Anomalous origin of the left coronary artery from the pulmonary artery
- Can occur in children or adults. In children it is said that 90% experience a myocardial infarct and die within 1st year of life - ALCAPA Syndrome in the Adult Patient
- To survive past infancy patients need to develop significant circulation from RCA to LCA
- Flow to LCA territory often insufficient and patient may develop malignant ventricular dysrhythmias which may result in sudden death - ALCAPA Syndrome in the Adult Patient: CTA Findings
- LCA arises from left inferolateral aspect of main pulmonary artery
- Secondary findings- - RCA and LCA may appear dilated and tortuous
- Dilated intercoronary collateral arteries may occur also in adults
- Left ventricular hypertrophy or dilatation may also occur
- ALCAPA Syndrome in the Pediatric Patient
- As pulmonary artery pressure drops after birth decreased flow to left ventricle myocardium
- This leads to congestive heart failure and mitral insufficiency secondary to myocardial infarction
- Patients will die within weeks of birth in 90% of cases w/o intervention - How do you quantify noncalcified plaque?
- CCTA allows detection of both calcified and non-calcified plaque
- Analysis of non-calcified plaque is used to determine luminal stenosis
- Non calcified plaque is typically only visible on contrast enhanced CT scans
- Is there an Agaston equivalent for non-calcified plaque
-
Severity of Coronary Artery Stenosis on CTA
Degree of StenosisDiameter Reduction (%)normalnone minimal1-25 mild26-50 moderate51-70 moderate71-99 occlusion100 Sundaram B, Kazerooni EA et al
AJR 2009;192:574-583 - Dominance of Coronary Circulation
- Dominance is determined by which branch gives rise to the atrioventricular nodal artery, the PDA and the posterolateral LV branches
- 80-85% of cases is right coronary dominant, 8-10% left coronary dominance and 7-8% codominance - "A large plaque size, densitometry performed not near the arterial lumen but at the center of the plaque, intracoronary enhancement of 250 H, and a low heart rate increase the accuracy of plaque densitometry."
Soft and Intermediate Plaques in Coronary Arteries: How Accurately Can We Measure CT Attenuation Using 64 MDCT?
Horiguchi J et al.
AJR 2007; 189:981-988 - "Coronary artery enhancement has a significant impact on 64-MDCT densitometry measurements of coronary artery plaques especially of soft plaques. A large plaque size, densitometry performed not near the arterial lumen but at the center of the plaque, intracoronary enhancement of 250 H, and a low heart rate increase the accuracy of plaque densitometry."
"Severe calcium artifacts were significantly reduced with dual-source CT."
Dual-Source Versus Single Source Cardiac CT Angiography:Comparison of Diagnostic Image Quality
Donnino R, Jacobs JE et al.
AJR 2009; 192:1051-1056"Dual-source CT provides significantly better diagnostic image quality than single source CT despite higher heart rates in the dual source CT Group. These findings support the use of dual-source CT for coronary artery imaging without the need for preexamination β-blockage."
Dual-Source Versus Single Source Cardiac CT Angiography:Comparison of Diagnostic Image Quality
Donnino R, Jacobs JE et al.
AJR 2009; 192:1051-1056"The primary results of our study reveal that the burden of angiographic disease detected by CTA provides both independent and incremental value in predicting all-cause mortality in symptomatic patients independent of age,gender,conventional risk factors and coronary artery calcification."
Mortality Incidence and the Severity of Coronary Atherosclerosis Assessed by Computed Tomography Angiography
Ostrom MP et al.
J Am Col Cardiol 2008 Oct 14;52916)1335-1343"To diagnose myocardial bridging in patients, sagittal multiplanar reconstruction images, in addition to axial images, should be evaluated."
Detection oF Myocardial Bridging with ECG-Gated MDCT and Multiplanar Reconstruction
Kantarci M et al.
AJR 2006; 186:S391-S394- How frequent a finding is it?
"Among the 626 patients, 22 cases (3.5%) of myocardial bridging were detected. Fifteen cases of myocardial bridging were located at the middle third of the left anterior descending coronary artery (LAD), five at the distal third of the LAD, and two at the proximal third of the LAD."
"In these patients the length of tunneled artery was between 6 and 22 mm, with a mean of 17 mm, and the depth of tunneled artery was between 1.2 and 3.3 mm, with a mean of 2.5 mm."Detection of Myocardial Bridging with ECG-Gated MDCT and Multiplanar Reconstruction
Kantarci M et al.
AJR 2006; 186:S391-S394 - " The coronary artery calcium (CAC) score above which it is recommended that coronary computerized tomographic angiography (CTA) not be performed has been steadily increasing. Currently, calcium scores > 1000 are thought to prohibit CTA accurate interpretation. However, a reasoned approach suggests that there is no absolute upper limit that applies to all patients and imaging centers."
How much calcium is too much calcium for coronary computerized tomographic angiography?
Hecht HS, Bhatti T
J Cardiovasc Comput Tomogr (2008) 2, 183-187
- " A CAC score of >1000 or a pattern of isolated large, dense calcifications with CAC < 1000 should alert personnel to potential interpretation problems and should not be followed by CTA if the interpreting physician does not have extensive experience in dealing with these issues.
How much calcium is too much calcium for coronary computerized tomographic angiography?
Hecht HS, Bhatti T
J Cardiovasc Comput Tomogr (2008) 2, 183-187
- " CCS (calcium coverage score) may enable better stratification of patients according to risk compared with the Agaston or mass score and thereby aid physicians in determining appropriate individual treatment strategies."
Coronary Calcium Coverage Score: Determination, Correlates, and Predictive Accuracy in the Multiethnic Study of Atherosclerosis
Brown ER et al.
Radiology 2008; 247:669-678
- " The calcium coverage score (CCS) was highly associated with coronary heart disease (CHD) events, and a twofold increase in CCS was associated with a 34% increase in the risk of any hard CHD event and a 52% increase in the risk of any CHD event."
Coronary Calcium Coverage Score: Determination, Correlates, and Predictive Accuracy in the Multiethnic Study of Atherosclerosis
Brown ER et al.
Radiology 2008; 247:669-678
- "Retten et al. have demonstrated that an important factor affecting measurement variability is the partial volume effect that operates when contiguous, rather than overlapping, scans are reconstructed. The practical implication of this error might be a false negative study or inaccurate categorization of the severity of patient risk."
Science to Practice: What is the Value of measuring Coronary Artery Calcification?
Wexler L
Radiology 246:1, Jan 2008;1-2
- "These large observational cohorts show that the absence of coronary artery calcification by Cardiac CT is associated with a low adverse risk and therefore could be used as a tool to counsel patients about the risk of such events."
Prognostic Significance of Zero Coronary Calcium Scores on Cardiac Computed Tomography
Shareghi S et al.
J Cardiovasc Comput Tomogr (2007)1, 155-159
- "Summary data show that in a total follow-up of 35,765 asymptomatic patients, 16,106 (45%) had scores of zero. Pooled sensitivity for CAC to detect a cardiovascular event was 98.1%, and negative predictive value was 99.9%."
Prognostic Significance of Zero Coronary Calcium Scores on Cardiac Computed Tomography
Shareghi S et al.
J Cardiovasc Comput Tomogr (2007)1, 155-159
- "In conclusion, asymptomatic persons without CAC (scores of zero) are shown to have a very low risk (0.27% per year) of future cardiovascular events during the subsequent 3-5 years and is a group unlikely to derive short term benefit from risk reducing pharmacotherapy."
Prognostic Significance of Zero Coronary Calcium Scores on Cardiac Computed Tomography
Shareghi S et al.
J Cardiovasc Comput Tomogr (2007)1, 155-159
- "Aortic calcification scores at CT colonography are significantly associated with established cardiac-related events. This screening information can be obtained without additional scanning or risk to the patient."
Assessment of Cardiovascular Risk Status at CT Colonography
Davila JA et al.
Radiology 2006; 240:110-115.
- " CT angiography was performed in 67 patients (50 male, 17 female; mean age 60.1 +/- 10.5 years) with suspected coronary artery disease and compared with invasive coronary angiography. All vessels >/=1.5 mm were considered for the assessment of significant coronary artery stenosis (diameter reduction >50%). Forty-seven patients were identified as having significant coronary stenoses on invasive angiography with 18% (176/1005) affected segments. None of the coronary segments needed to be excluded from analysis. CT correctly identified all 20 patients having no significant stenosis on invasive angiography. Overall sensitivity for classifying stenoses was 94%, specificity was 97%, positive predictive value was 87%, and negative predictive value was 99%."
- Material and Methods: Overall sensitivity for classifying stenoses was 94%, specificity was 97%, positive predictive value was 87%, and negative predictive value was 99%."
Conclusion: Sixty-four-slice CT provides a high diagnostic accuracy in assessing coronary artery stenoses.
Accuracy of MSCT coronary angiography with 64-slice technology: first experience.
Leschka S et al. Eur Heart J. 2005 Apr 19; [Epub ahead of print
- " The currently best available spatial and temporal resolution for retrospectively ECG gated coronary multi-detector-row CT angiography is 0.4 mm and 165 ms, respectively. These acquisition parameters are already rather close to cardiac catheter. Studies so far compared non-invasive coronary CT and convention angiography for the detection of coronary artery stenoses. The most promising result reported by all authors was the high negative predictive value of the CTA."
Coronary CT angiography in symptomatic patients
Becker CR.
Eur Radiol. 2005 Feb;15 Suppl 2:B33-41
- "The most promising result reported by all authors was the high negative predictive value of the CTA."
Coronary CT angiography in symptomatic patients
Becker CR.
Eur Radiol. 2005 Feb;15 Suppl 2:B33-41
- " CT Angiography is more accurate than calcium scoring in demonstrating coronary artery stenosis. A patient calcium score of greater than or equal to 400, however, can be used to potentially identify patients with significant coronary stenoses not detected at CT angiography."
Coronary Artery Stenosis: Detection with Calcium Scoring, CT Angiography, and Both Methods Combined
Lau GT et al.
Radiology 2005; 235:415-422
- " Combining CT angiography with Calcium Scoring (over 400) improved the sensitivity of CT angiography (from 93 to s100%) in demonstrating significant coronary disease in patients."
Coronary Artery Stenosis: Detection with Calcium Scoring, CT Angiography, and Both Methods Combined
Lau GT et al.
Radiology 2005; 235:415-422
- "In a population having a low pretest likelihood of significant coronary artery disease, 16-MDCT shows a moderate to high sensitivity and a high NPV for the detection or exclusion of significant disease, but has a somewhat reduced PPV compared with conventional coronary angiography."
Clinical Value of MDCT in the Diagnosis of Coronary Artery Disease in Patients with a Low Pretest Likelihood of Significant Disease
Nikolaou K et al.
AJR 2006;186:1659-1668.
- "Although 16-MDCT appeared to overestimate diagnoses as compared with QCA, resulting in a relatively high number of false-positive diagnosis of significant coronary artery disease, this may have been a consequence either of the relatively small patient population or of false negative diagnosis on QCA."
Clinical Value of MDCT in the Diagnosis of Coronary Artery Disease in Patients with a Low Pretest Likelihood of Significant Disease
Nikolaou K et al.
AJR 2006;186:1659-1668.
- "CTA has the potential to perform cross-sectional imaging through the narrowed portion of the lumen and to measure the area of the vessel lumen versus the area of an adjacent,apparently normal segment, which are not possible using QCA."
Clinical Value of MDCT in the Diagnosis of Coronary Artery Disease in Patients with a Low Pretest Likelihood of Significant Disease
Nikolaou K et al.
AJR 2006;186:1659-1668.
- Opinion
- False positive coronary CTA is less of a practical issue that false negative coronary CTA. The lack of false negative is especially critical
- "Sensitivity, specificity, and the negative predictive value (NPV) of 64-MDCT per patient were 97%, 79%, and 96%, respectively. Per segment, 923 of 1,020 coronary artery segments were assessable (90%). For the detection of stenoses of more than 50% and more than 75% per segment, 64-MDCT showed a sensitivity of 82% and 86%, respectively. Per segment, specificity and NPV were as high as 95% and 97%, respectively."
Accuracy of 64-MDCT in the diagnosis of ischemic heart disease
Nikolaou K et al
AJR 2006 July; 187(1):111-117.
- "Significant stenosis was defined as a diameter reduction of > 50%. Of 966 segments, 884 (92%) were assessable. Compared with ICAG, the sensitivity of CTA to diagnose significant stenosis was 90%, specificity 94%, positive predictive value (PPV) 89% and negative predictive value (NPV) 95%."
Diagnostic accuracy of 64-slice computed tomography for detecting angiographically significant coronary artery stenosis in an unselected consecutive patient population: comparison with conventional invasive angiography.
Ehara M et al.
Circ J 2006 May; 70(5):564-571.
- "On 64-MDCT, 89% of coronary artery segments are assessible. Ten or more vessel segments are assessable in 94% of patients."
Coronary CT Angiography with 64-MDCT: Assessment of Vessel Visibility
Pannu HK,Jacobs JE,Lai S,Fishman EK
AJR 2006; 187:119-128.
- "In clinical routine, coronary CTA will primarily be used for risk stratification on a per patient basis. In the present study, coronary 64-MDCT showed a high diagnostic accuracy on both per patient and per segment analyses."
Accuracy of 64-MDCT in the Diagnosis of Ischemic Heart Disease
Nikolaou K et al.
AJR 2006; 187:111-117.
- "In conclusion, 64 MDCT coronary angiography provides a significantly increased spatial and temporal resolution compared with earlier MDCT systems. In a clinical setting, this technique may hold great promise for the reliable diagnosis or exclusion of significant CAD on a per patient basis and could give CTA an important role in the stratification of patients with both known and suspected CAD."
Accuracy of 64-MDCT in the Diagnosis of Ischemic Heart Disease
Nikolaou K et al.
AJR 2006; 187:111-117.
- "68 of 72 coronary CT angiograms (94%) were of diagnostic image quality. QCA showed significant CAD (i.e. one or more stenosis in >50%) in 57% (39/68) and nonsignificant disease or healthy CTA’s in 43% (29/68) of the patients. Sensitivity, specificity and the negative predictive value of 64 MDCT per patient were 97%, 79%, and 96% respectively."
Accuracy of 64-MDCT in the Diagnosis of Ischemic Heart Disease
Nikolaou K et al.
AJR 2006; 187:111-117.
- Plaque Attenuation Scoring
- Predominantly lipid rich plaques; < 60HU
- Intermediate plaques: 61-119 HU
- Predominately calcified plaques: >120 HU
- Reliability of Differentiating Human Coronary Plaque Morphology Using
- Contrast Enhanced Multislice Spiral Computed Tomography
Schroeder S et al.
J Comput Assist Tomogr 2004;28:449-454
- " The finding may have implications for the interpretation of calcification of atherosclerotic plaque in other vascular beds."
Calcified Carotid Atherosclerotic Plaque Is Associated Less with Ischemic Symptoms Than Is Noncalcified Plaque on MIDST
Nandalur KR et al.
AJR 2005;184;295-298
- " Image attenuation values vary by scanner and participant body size, producing calcium score differences that are not due to true calcium burden disparities. Use of calibration phantoms may improve the comparability of such measurements between persons scanned with different scanners and within persons over time."
Measuring Coronary Calcium on CT images Adjusted for Attenuation Differences
Nelson JC et al.
Radiology 2005;235:404-414
- " Micro CT provides quantitative information about plaque morphology equivalent to that provided with histomorphometric analysis. Micro CT is feasible for analysis of the coronary artery wall."
Atherosclerotic Lesions at Micro CT: Feasibility for Analysis of Coronary Artery Wall in Autopsy Specimens
Langheinrich AC et al.
Radiology 2004; 231:675-681
- " The absence of detectable calcium does not reliably exclude substantial coronary disease."
Coronary Artery Stenosis: Detection with Calcium Scoring, CT Angiography, and Both Methods Combined
Lau GT et al.
Radiology 2005; 235:415-422
- " The accuracy of sequential MDCT for coronary calcium quantification is sufficient in most cases for stratification of patient risk."
Potential Clinical Impact of Variability in the Measurement of Coronary Artery Calcification with Sequential MDCT
Halliburton SS et al.
AJR 2005; 184:643-648
- "Differences in coronary artery calcium measurements using EBT and MDCT are similar to interscan differences in CAC measurements previously reported for EBT or for other MDCT scanners individually."
Concordance of Coronary Artery Calcium Estimates Between MDCT and Electron Beam Tomography Daniell AL et al. AJR 2005; 185:1542-1545
- "Electron beam and multidetector row CT scanners have equivalent reproducibility for measuring coronary artery calcium. Calcium volumes and interpolated volume scores are slightly more reproducible than Agatston scores."
Coronary Calcium Measurements: effect of CT Scanner Type and Calcium Measure on Rescan reproducibility-MESA Study Detrano RC et al. Radiology 2005; 236:477-484
- "MDCT is a promising tool for coronary calcium scoring; however, more studies are needed comparing EBCT and MDCT, especially at lower coronary artery calcium levels."
Electron beam CT versus helical CT scans for assessing coronary calcifications: Current utility and future directions
Nasir K, Budoff M, Post WS, Fishman EK, Mahesh M, Lima JA, Blumenthal RS
Am Heart J 2003; 146:969-977.
- "For a true exclusion of coronary artery calcifications, different reconstruction intervals have to be evaluated."
Different Reconstruction Intervals for Exclusion of Coronary Artery Calcifications by Retrospectively Gated MDCT
Sandstede JJW et al.
AJR 2006; 186:193-197(4 slice MDCT).
- "Whereas in the present study 69-77% of patients with a low pretest probability for the presence of CAD had a calcium score of 0 at one reconstruction interval at least, in only 42% of the patients could coronary artery calcification be excluded after evaluation of all reconstructions at 50%,60%,70%, and 80% of the R-R interval."
Different Reconstruction Intervals for Exclusion of Coronary Artery Calcifications by Retrospectively Gated MDCT
Sandstede JJW et al.
AJR 2006; 186:193-197(4 slice MDCT).
- "Electron-beam and multi-detector row CT scanners have equivalent reproducibility for measuring coronary artery calcium. Calcium volumes and interpolated volume scores are slightly more reproducible than Agaston scores. Reproducibility is lower for scans with misregistrations or motion artifacts."
Coronary Calcium measurements: Effect of CT Scanner Type and Calcium Measure on Rescan Reproducibility-MESA Study
Detrano RC et al.
Radiology 2005; 236:477-484.
- Factoid
- A zero coronary calcification score is associated with a high negative predictive value (nearly 100%) for excluding hemodynamically relevant CAD. The score must be 0 not 1,2 or 3 Agaston units.