“The abdominal aorta supplies paired lumbar arteries at multiple levels posteriorly, paired renal arteries laterally, paired common iliac arteries inferiorly, and 3 visceral arteries anteriorly: the celiac artery, superior mesenteric artery (SMA), and inferior mesenteric artery (IMA ). In 65% to 75% of patients, the celiac artery gives rise to the left gastric artery (LGA) and then bifurcates into the common hepatic (CHA) and splenic arteries. The CHA gives rise to the gastroduodenal artery (GDA) and becomes the proper hepatic artery;bthis splits into right hepatic artery (RHA) and left hepatic artery (LHA) branches in 55% of patients. Several collateral pathways interconnect the visceral arteries: pancreaticoduodenal artery(PDA) anastomosis (GDA-SMA), arc of Buhler (celiac-SMA), arc of Barkow (gastroepiploic anastomosis),marginal artery of Drummond (SMA-IMA), and arc of Riolan (SMA-IMA)..”
Imaging of Visceral Vessels
Theodore T. Pierce, MD, MPHa,*, Vinay Prabhu, MD, MSb, Vinit Baliyan, MDc, Sandeep Hedgire, MDc
Radiol Clinics N A 2024 (in press)
“Variant hepatic arterial anatomy (arteries from a nonstandard vessel [replaced] or supernumerary vessels supplying less than a liver lobe [accessory]) affects the surgical approach in liver transplantation, tumor resection, intra-arterial therapy, and other surgical situations. Variants include accessory LHA (incidence 8%–13%) and replaced LHA (10%–12%) from the LGA4 and replaced CHA (2.5%), replaced RHA (10%–17%), or accessory RHA (6%–8%) from the SMA. Combinations of these variants may be present.”
Imaging of Visceral Vessels
Theodore T. Pierce, MD, MPHa,*, Vinay Prabhu, MD, MSb, Vinit Baliyan, MDc, Sandeep Hedgire, MDc
Radiol Clinics N A 2024 (in press)
Ehlers-Danlos syndrome (EDS; prevalence 1:5000–250,00011) is a collection of 11 distinct connective tissue diseases. Vascular EDS (4% of EDS), formerly EDS type IV, is an AD defect in type III procollagen. Vascular fragility predisposes to vascular ectasia, aneurysm, and dissection, typically multifocal, involving the aorta, head/ neck, splanchnic, and iliac arteries with resulting target organ (such as renal, splenic, or brain) hemorrhage, ischemia, or infarcts. Aortic root involvement is uncommon Patients are at risk of uterine and intestinal rupture. Patients often have complications as young adults, up to 80% by the age of 40 years, but are often undiagnosed at the time of their first vascular event.
Imaging of Visceral Vessels
Theodore T. Pierce, MD, MPHa,*, Vinay Prabhu, MD, MSb, Vinit Baliyan, MDc, Sandeep Hedgire, MDc
Radiol Clinics N A 2024 (in press)
Aortic occlusion results from embolism (acute or chronic) or thrombosis (due to atherosclerosis and smoking). This can be recognized by the development of extensive collaterals from the lower thoracic/upper abdominal arteries to the iliac/ femoral arteries, such as the pathway of Winslow (internal mammary to inferior epigastric arteries), which supply the lower extremities in this setting. Chronic infrarenal aortic occlusion may present with characteristic symptoms, Leriche syndrome (buttock claudication, impotence, and/ or diminished femoral pulses).
Imaging of Visceral Vessels
Theodore T. Pierce, MD, MPHa,*, Vinay Prabhu, MD, MSb, Vinit Baliyan, MDc, Sandeep Hedgire, MDc
Radiol Clinics N A 2024 (in press)
“Fibromuscular dysplasia (FMD) is a surprisingly common (prevalence 3.34%), noninflammatory and nonatherosclerotic medium-vessel arteriopathy typically involving renal (67% of patients with FMD), iliac (32%), and mesenteric arteries (22%). Ninety percent of cases present in women aged 20 to 60 years. Imaging findings of FMD include arterial beading, stenosis, aneurysm, dissection (including spontaneous coronary artery dissection), tortuosity, occlusion, and end organ ischemia. Multivessel involvement is common; however, aortic involvement is unusual. Vascular findings, such as mural irregularity, may be subtle, requiring high-resolution CT angiography with MIPs, MPRs, and CPRs for detection Imaging findings of vasculitis and FMD are similar, although systemic inflammation would suggest vasculitis. Multiple dissections raise the possibility of Marfan syndrome, LDS, or vascular EDS, although characteristic clinical/physical examination findings may distinguish genetic syndromes from FMD.”
Imaging of Visceral Vessels
Theodore T. Pierce, MD, MPHa,*, Vinay Prabhu, MD, MSb, Vinit Baliyan, MDc, Sandeep Hedgire, MDc
Radiol Clinics N A 2024 (in press)
Segmental arterial mediolysis (SAM) is a rare idiopathic noninflammatory medium vessel arteriopathy most often affecting middle-aged and elderly men. SAM causes arterial dissection (71%–86%), aneurysm (43%–57%), stenosis, occlusion, spontaneous hemorrhage, and ischemia, often with multivessel involvement.29–31 Presenting symptoms include abdominal pain (50%– 74%) and hemorrhagic shock (32%) due to vessel rupture. Visceral dissecting aneurysms, segmental mural soft tissue thickening (rind sign), and occlusion affect the renal arteries, SMA, and celiac trunk (each in half of patients) and less frequently the hepatic, iliac, and splenic arteries. Visceral vessel branch sites and aortic involvement are unusual. Differentiating SAM and FMD is difficult; in fact, some consider SAM an FMD-precursor, an FMD-variant, or the samedisease as FMD.
Imaging of Visceral Vessels
Theodore T. Pierce, MD, MPHa,*, Vinay Prabhu, MD, MSb, Vinit Baliyan, MDc, Sandeep Hedgire, MDc
Radiol Clinics N A 2024 (in press)
Visceral artery aneurysms involve the splenic (w35%;), celiac (30%), hepatic (13%– 20%), and PDA (2%–10%) arteries. Managementdepends on the vessel involved, size, mural integrity, and cause. Causes of true aneurysms include atherosclerosis, FMD, cystic medial necrosis, and portal hypertension. The principal risk, aneurysm rupture, is considered low when less than 2 cm. Some suggest following aneurysms up to 2.5 cm by imaging every 1 to 3 years because change in size is uncommon. Patients who are pregnant or planning pregnancy undergo splenic artery aneurysm repair regardless of size due to the maternal (75%) and fetal (95%) mortality associated with rupture. PDA and GDA aneurysms are repaired due to risk of rupture (w20%) despite small size (20% of ruptured aneurysms are <20 mm). PDA/GDA aneurysms often occur with celiac artery narrowing or occlusion resulting in an increased GDA/PDA flow, wall shear stress, and rupture risk.
Imaging of Visceral Vessels
Theodore T. Pierce, MD, MPHa,*, Vinay Prabhu, MD, MSb, Vinit Baliyan, MDc, Sandeep Hedgire, MDc
Radiol Clinics N A 2024 (in press)
“May-Thurner syndrome (iliac vein compression syndrome) is left common iliac vein compression by the right common iliac artery50 (or left common iliac artery in the variant form) leading to left lower extremity swelling and thrombogenesis. Women (5:1) aged 10 to 40 years are mainly affected.50 Imaging findings includeleft iliac vein compression ( 50%narrowing), cross pelvic collaterals, left internal iliac vein flow reversal on time of flight MR imaging, and venous thrombosis. Correct diagnosis is difficult without measurement of a pressure gradient because compression alone is common (25% of patients) and may resolve simply with hydration.”
Imaging of Visceral Vessels
Theodore T. Pierce, MD, MPHa,*, Vinay Prabhu, MD, MSb, Vinit Baliyan, MDc, Sandeep Hedgire, MDc
Radiol Clinics N A 2024 (in press)
PVG has a high mortality (56%–90%) due to frequent association with bowel necrosis (72%), although early detection and treatment can decrease mortality. Intramural bowel gas, pneumatosis intestinalis, from bowel necrosis can dissect into draining veins and lead to PVG. PVG is apparent on radiograph (branching intrahepatic lucency), US (nondependent echogenic flowing intravascular particles), and CT (intravascular gas within the mesenteric veins or PV). Pneumobilia mimics PVG; however, PVG is typically peripheral while pneumobilia is central; tracing the respective structures on sequential images is helpful. Notably, numerous benign causes of PVG exist.
Imaging of Visceral Vessels
Theodore T. Pierce, MD, MPHa,*, Vinay Prabhu, MD, MSb, Vinit Baliyan, MDc, Sandeep Hedgire, MDc
Radiol Clinics N A 2024 (in press)
To achieve optimal aortic visualization, an opacification exceeding 250 Hounsfield units (HU)— ideally surpassing 300 HU—is advised. Typically, an iodinated contrast medium is administered at a flow rate of 3 to 6 mL/s, using a total volume between 100 and 125 mL. This is subsequently followed by a 40 mL normal saline flush at a rate of 4 mL/s. The post-contrast image acquisition is either automated through bolus tracking software or manually set using a test bolus, which typically involves 15 to 20 mL of contrast. Given the ease of use, the automated contrast bolus tracking software is preferred over the test bolus method. In addition, it involves reduced contrast doses and an enhanced signal-to-background ratio, ensuring no inadvertent opacification of parenchymal organs from test dose contrast.
Computed Tomography Angiography for Aortic Diseases
Ishan Garg et al.
Radiol Clin N Am - (2024) -–-
https://doi.org/10.1016/j.rcl.2024.01.001On the other hand, VR images are created from 3D data sets by utilizing predetermined density thresholds. This is particularly useful in distinguishing between intraluminal contrast and stent materials, given that stent materials usually exhibit a higher density compared to intraluminal contrast. MIP images preferentially display only the highest density pixels from the data into a single plantar image. This allows excellent visualization of a highdensity material such as contrast, calcification, endograft, and collateral circulation (in scenarios with vascular occlusion or pronounced stenosis).
Computed Tomography Angiography for Aortic Diseases
Ishan Garg et al.
Radiol Clin N Am - (2024) -–-
https://doi.org/10.1016/j.rcl.2024.01.001 An acute PAU occurs due to the ulceration of an atherosclerotic plaque deep into the arterial wall. It accounts for 2% to 7% of all AAS and affects elderly patients with severe atherosclerotic disease. It is most commonly located in the descending thoracic aorta. Clinically acute PAU presents similar to aortic dissection and other AAS. Acute PAU can be associated with IMH from hemorrhage in the media and can progress to frank aortic dissection (intimomedial tear with true and false lumen), aneurysm, or rupture (penetrating through all 3 layers of the aortic wall resulting in saccular, fusiform, or pseudoaneurysm, which may ultimately rupture) based on level of penetration. Overall, rupture is uncommon.
Computed Tomography Angiography for Aortic Diseases
Ishan Garg et al.
Radiol Clin N Am - (2024) -–-
https://doi.org/10.1016/j.rcl.2024.01.001 The most widely used classification system used for grading the severity of BTTAI was developed by Azizzadeh and colleagues in 2009, and since then, it has been endorsed by the Society for Vascular Surgery clinical practice guidelines.
Grade 1: Intimal tear, intimal flap, or both.
Grade 2: Intramural hematoma
Grade 3: Aortic wall disruption with pseudoaneurysm
Grade 4: Aortic wall disruption with free rupture
Grade 1 and 2 BTTAIs can be managed with either a nonoperative or operative approach. In contrast, the severity of Grade 3 and 4 injuries typically necessitates prompt, definitive management using endovascular repair. Frequently, the term, “minimal aortic injury” is used for sub-centimeter intimo-medial abnormality with no external contour deformity.
Computed Tomography Angiography for Aortic Diseases
Ishan Garg et al.
Radiol Clin N Am - (2024) -–- https://doi.org/10.1016/j.rcl.2024.01.001
True aneurysm vs. pseudoaneurysms
- A true aneurysm is characterized by dilation and thinning of the entirety of the vessel wall [11] greater than 1.5 times the expected vessel diameter and includes all three tunicae of the artery.
- Pseudoaneurysms are typically the result of a traumatic disruption of the intimal and medial layers of the vessel with the aneurysm contained by the adventitia and/or perivascular tissues only.
True aneurysm vs. pseudoaneurysms
Distinguishing between the two true aneurysms and pseudoaneurysms is important as the clinical course and complication rates differ significantly between them. In particular, the rate of rupture in pseudoaneuryms has been reported to be much higher than true aneurysms.
Normal Artery Size
- Celiac trunk, 0.79 ± 0.06 cm
- Common hepatic artery, 0.50 ± 0.04 cm
- Proper hepatic artery, 0.45 ± 0.03 cm
- Splenic artery, 0.46 ± 0.03 cm
Visceral Artery Aneurysms: Facts
Splenic artery aneurysms are the most common VAAs, representing 60–70% of all VAAs. Significantly less common are hepatic artery aneurysms and celiac/ mesenteric artery aneurysms, which comprise 20 and 10% of VAAs, respectively [2]. Splenic artery aneurysms are most common among multiparous women, while hepatic and gastroduodenal arteries are more common in men. Celiac and superior mesenteric artery aneurysms have been reported equally among both sexes .
Visceral Artery Aneurysms: Facts
Etiologies for VAAs include atherosclerosis (most common, 32%), vasculitis, collagen vascular disease, infection, fibromuscular dysplasia, trauma (22%), and iatrogenic and idiopathic causes. Multiple aneurysms are found in up to one third of patients and are frequently associated connective tissue or collagen vascular diseases.
Visceral Artery Aneurysms: Treatment
- Symptomatic aneurysms are also at high risk for rupture and should be treated whenever possible.
- Conservative management is reasonable for most asymptomatic aneurysms under 2cm
- Aneurysms that are greater than 2 cm usually warrant therapy as studies performed in patients with VAAs indicate that rupture is more likely when aneurysm diameter is greater than 2–2.5 cm .
- Calcified aneurysms are thought to be an indicator of chronicity and stability. As a result, many practitioners manage calcified aneurysms conservatively especially in patients at increased surgical and procedural risk.
“In our own experience, 3D reconstruction methods can be invaluable for the assessment of small bowel abnormalities; in particular, the 2 most important reconstruction methods are (1) maximum intensity projection (MIP) imaging, and (2) volume rendering (VR). MIP imaging entails us- ing a computer algorithm to acquire the highest attenuation voxels in a data set and to project these high-attenuation voxels into a 3D display that can be manipulated by the radiologist. These reconstructions are invaluable in the assessment of the mesenteric vasculature (including the small second-order and third-order branch vessels, which can be visualized on the latest generations of scanners), and can accentuate vascular abnor- malities that may not be readily appreciated on the source axial images.”
Computed Tomography Angiography of the Small Bowel and Mesentery
Raman SP,Fishman EK
Radiol Clin N Am 54 (2016) 87–100
“MIP imaging entails using a computer algorithm to acquire the highest attenuation voxels in a data set and to project these high-attenuation voxels into a 3D display that can be manipulated by the radiologist. These reconstructions are invaluable in the assessment of the mesenteric vasculature (including the small second-order and third-order branch vessels, which can be visualized on the latest generations of scanners), and can accentuate vascular abnormalities that may not be readily appreciated on the source axial images.”
Computed Tomography Angiography of the Small Bowel and Mesentery
Raman SP,Fishman EK
Radiol Clin N Am 54 (2016) 87–100
“VR is a much more computationally complex process (it is beyond the scope of this article) but, in simple terms, it involves using a computer algorithm to assign a specific color and transparency to each voxel in a data set based on both its attenuation and its relationship to adjacent voxels, and then using this information to create an interactive 3D display. VR techniques are more valuable for assessing the bowel wall itself (rather than the vasculature), and can nicely show the 3D relationships of adjacent organs and structures.”
Computed Tomography Angiography of the Small Bowel and Mesentery
Raman SP,Fishman EK
Radiol Clin N Am 54 (2016) 87–100
OBJECTIVES: (1) To evaluate the ability of emergency room radiologists to detect acute mesenteric ischemia (AMI) from computed tomography (CT) images in patients with acute abdominal pain. (2) To identify factors affecting radiologists' performance in the CT interpretation and patient outcome.
CONCLUSIONS: AMI is underdiagnosed in the CT of the acute abdomen if there is no clinical suspicion.
Detecting acute mesenteric ischemia in CT of the acute abdomen is dependent on clinical suspicion: Review of 95 consecutive patients.
Lehtimäki TT et al.
Eur J Radiol. 2015 Sep 11. pii: S0720-048X(15)30098-X. doi: 10.1016/j.ejrad.2015.09.006. [Epub ahead of print]
“The referring clinician had suspected AMI in 30 (31%) cases prior to imaging. The crucial findings of AMI had been stated in 97% of the radiology reports if the clinician had mentioned AMI suspicion in the referral; if not, the corresponding rate was 81% (p=0.04). Patients without suspicion of AMI prior to CT were more prone to undergo bowel resection. CT protocol was optimal for AMI (with contrast enhancement in arterial and venous phases) in only 34 (35%) cases. Intestinal findings were more difficult to detect than vascular findings. Vascular findings were retrospectively detectable in 92% of cases with embolism and 100% in ASVD and MVT.
Detecting acute mesenteric ischemia in CT of the acute abdomen is dependent on clinical suspicion: Review of 95 consecutive patients.
Lehtimäki TT et al.
Eur J Radiol. 2015 Sep 11. pii: S0720-048X(15)30098-X. doi: 10.1016/j.ejrad.2015.09.006. [Epub ahead of print]
“The referring clinician had suspected AMI in 30 (31%) cases prior to imaging. The crucial findings of AMI had been stated in 97% of the radiology reports if the clinician had mentioned AMI suspicion in the referral; if not, the corresponding rate was 81% (p=0.04).
Detecting acute mesenteric ischemia in CT of the acute abdomen is dependent on clinical suspicion: Review of 95 consecutive patients.
Lehtimäki TT et al.
Eur J Radiol. 2015 Sep 11. pii: S0720-048X(15)30098-X. doi: 10.1016/j.ejrad.2015.09.006. [Epub ahead of print]
“The referring clinician had suspected AMI in 30 (31%) cases prior to imaging. The crucial findings of AMI had been stated in 97% of the radiology reports if the clinician had mentioned AMI suspicion inn the referral; if not, the corresponding rate was 81% (p=0.04). Patients without suspicion of AMI prior to CT were more prone to undergo bowel resection. CT protocol was optimal for AMI (with contrast enhancement in arterial and venous phases) in only 34 (35%) cases.”
Detecting acute mesenteric ischemia in CT of the acute abdomen is dependent on clinical suspicion: Review of 95 consecutive patients.
Lehtimäki TT et al.
Eur J Radiol. 2015 Sep 11. pii: S0720-048X(15)30098-X. doi: 10.1016/j.ejrad.2015.09.006. [Epub ahead of print]
“Vascular findings were retrospectively detectable in 92% of cases with embolism and 100% in ASVD and MVT. Some evidence of intestinal abnormality was retrospectively found in the CT findings in 92%, 100%, 100% and 67% of cases with embolism, ASVD, NOMI and MVT, respectively.”
Detecting acute mesenteric ischemia in CT of the acute abdomen is dependent on clinical suspicion: Review of 95 consecutive patients.
Lehtimäki TT et al.
Eur J Radiol. 2015 Sep 11. pii: S0720-048X(15)30098-X. doi: 10.1016/j.ejrad.2015.09.006. [Epub ahead of print]
“CTA can also be helpful in stratifying patients to identify those who would benefit from angiography as opposed to the ones who should undergo emergent surgery. Vascular CT findings include arterial stenosis, embolism, thrombosis, arterial dissection, and mesenteric vein thrombosis; nonvascular CT findings include bowel wall thickening, hypoperfusion and hypoattenuation, bowel dilatation, bowel wall hemor- rhage, mesenteric fat stranding, pneumatosis intesti- nalis, and portal venous gas. Overall, combining vascular findings with the appearance of the bowel wall resulted in a specificity of 94% with a sensitivity of 96%.”
ACR appropriateness criteria imaging of mesenteric ischemia
Oliva IB et al.
Abdom Imaging (2013) 38:714–719
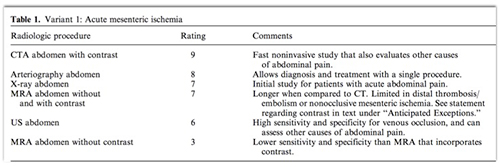
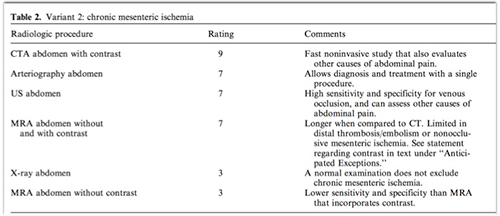
“Mesenteric ischemia is a rare disease associated with high morbidity and mortality. Acute mesenteric ischemia is most commonly secondary to embolism followed by arterial thrombosis, nonocclusive ischemia, and less commonly venous thrombosis. Chronic mesenteric ischemia is almost always caused by atherosclerotic disease, with rare causes including fibromuscular dysplasia and vasculitis.”
ACR appropriateness criteria imaging of mesenteric ischemia
Oliva IB et al.
Abdom Imaging (2013) 38:714–719
“Acute mesenteric ischemia is most commonly secondary to embolism to the superior mesenteric artery (SMA), which accounts for approximately 40%–50% of all episodes. Acute mesenteric artery thrombosis is the second most common cause of acute mesenteric ischemia (20%–30%) followed by nonocclusive mesenteric ischemia (25%) and less commonly mesenteric and portal venous thrombosis (5%–15%).”
ACR appropriateness criteria imaging of mesenteric ischemia
Oliva IB et al.
Abdom Imaging (2013) 38:714–719
“Mesenteric and portal venous thrombosis is the least common cause of acute mesenteric ischemia. Most common risk factors are hypercoagulable states, portal hypertension, and recent surgery. Bowel ischemia occurs if there is no adequate collateral circulation to drain the intestinal mucosa, leading to edema and subsequent arterial hypoperfusion.”
ACR appropriateness criteria imaging of mesenteric ischemia
Oliva IB et al.
Abdom Imaging (2013) 38:714–719
“Computed tomography angiography (CTA) is a fast and noninvasive test with high sensitivity and specificity in diagnosing acute and chronic mesenteric ischemia and should be considered the first-line test in most cases. CT imaging of the abdomen also allows accu- rate evaluation of the entire gastrointestinal and genitourinary tract, helping to exclude most of the other causes of acute and chronic abdominal pain, including cholelithiasis, cholecystitis, pancreatitis, appendicitis, diverticulosis with or without diverticulitis, and nephrolithiasis.”
ACR appropriateness criteria imaging of mesenteric ischemia
Oliva IB et al.
Abdom Imaging (2013) 38:714–719
“CTA with 3D volume reformatting has sensitivity and specificity of 96% and 94%, respectively, for detecting chronic mesenteric ischemia. Therefore, it should be considered as a first-line alternative to angiography for diagnostic purposes. Moreover, CTA is an accurate diagnosing tool for detecting SMA syndrome. CT can also accurately exclude other causes of chronic abdominal pain.”
ACR appropriateness criteria imaging of mesenteric ischemia
Oliva IB et al.
Abdom Imaging (2013) 38:714–719
“CTA is an emerging diagnostic test with high sensitivity and specificity in the setting of both acute and chronic mesenteric ischemia and should be considered the first-line imaging test. CT can also accurately assess for other causes of acute and chronic abdominal pain, and it provides excellent anatomic mapping of the mesenteric vasculature, which is essential in the preoperative planning.”
ACR appropriateness criteria imaging of mesenteric ischemia
Oliva IB et al.
Abdom Imaging (2013) 38:714–719
Segmental Arterial Mediolysis: Facts
- Middle aged to elderly patient (age 50-80)
- Leading cause of spontaneous intra-abdominal hemorrhage
- May present with abdominal pain, distension, dropping hematocrit or shock
- Mortality as high as 50%
Segmental Arterial Mediolysis: CT Findings
- Fusiform aneurysms
- Arterial stenosis
- Vessel dissections
- Vessel occlusions
- Spontaneous hemorrhage may be seen
Segmental Arterial Mediolysis: Differential Diagnosis
- Polyarteritis nodosa, Wegener’s granulomatosis
- Mycotic aneurysms
- Cystic medial necrosis
- Fibromuscular dysplasia
“Diagnosis of acute mesenteric ischaemia in the early stages is now possible with modern computed tomography (CT), using intravenous contrast enhancement and imaging in the arterial and/or portal venous phase. The availability of CT around the clock means that more patients with acute mesenteric ischaemia may be treated with urgent intestinal revascularization.”
Modern treatment of acute mesenteric ischaemia.
Br J Surg. 2014 Jan;101(1):e100-8
Acosta S, Björck M
“Endovascular therapy has become an important alternative, especially in patients with acute thrombotic superior mesenteric artery (SMA) occlusion, where the occlusive lesion can be recanalized either antegradely from the femoral or brachial artery, or retrogradely from an exposed SMA after laparotomy, and stented. Aspiration embolectomy, thrombolysis and open surgical embolectomy, followed by on-table angiography, are the treatment options for embolic SMA occlusion. Endovascular therapy may be an option in the few patients with mesenteric venous thrombosis who do not respond to anticoagulation therapy. Laparotomy is needed to evaluate the extent and severity of visceral organ ischaemia, which is treated according to the principles of damage control surgery.”
Modern treatment of acute mesenteric ischaemia.
Br J Surg. 2014 Jan;101(1):e100-8
Acosta S, Björck M
“ Percutaneous revascularization is a promising alternative to surgery for acute SMA occlusion in selected patients who have no signs of advanced bowel ischemia. Early diagnosis followed by prompt endovascular intervention with close postprocedural monitoring is key. Laparotomy is indicated in patients who develop new or worsening signs of peritonism after endovascular procedure, particularly in those who had complete occlusion of the main trunk of the SMA.”
Early endovascular treatment of superior mesenteric occlusion secondary to thromboemboli.
Jia Z et al.
Eur J Vasc Endovasc Surg. 2014 Feb;47(2):196-203.
“ Computed tomography angiography revealed complete occlusion in seven cases and incomplete occlusion in 14 cases, with no evidence of free gas or bowel necrosis. The median duration from onset of symptoms to revascularization was 8.7 ± 4.1 hours (range, 2-18 hours). Completely successful endovascular revascularization occurred in six cases (aspiration alone, 3 cases; combined aspiration and urokinase, 3 cases); partial success was achieved in 15 cases (aspiration alone, 4 cases; combined aspiration and urokinase, 10 cases; and combined aspiration, urokinase, and stent placement, 1 case). Laparotomy was required in five patients, all of whom had SMA main trunk complete occlusion and required small bowel resection.”
Early endovascular treatment of superior mesenteric occlusion secondary to thromboemboli.
Jia Z et al.
Eur J Vasc Endovasc Surg. 2014 Feb;47(2):196-203.
“The 30-day mortality for all patients was 9.5%. During a median follow-up of 26 months, 15 patients remained asymptomatic, three patients reported occasional abdominal pain, and one patient had temporary short-bowel syndrome.”
Early endovascular treatment of superior mesenteric occlusion secondary to thromboemboli.
Jia Z et al.
Eur J Vasc Endovasc Surg. 2014 Feb;47(2):196-203.
PURPOSE: The goals of this study were to investigate the treatment outcomes of acute mesenteric ischemia caused by superior mesenteric artery (SMA) embolism and identify the posttreatment prognostic factors.
CONCLUSIONS: Prompt diagnosis and treatment before extensive irreversible gangrene is the mainstay in the treatment of SMA embolism. Limited bowel gangrene was not associated with mortality.
Treatment outcome in patients with acute superior mesenteric artery embolism.
Yun WS et al.
Ann Vasc Surg. 2013 Jul;27(5):613-20.
INTRODUCTION: Acute mesenteric ischemia (AMI) is a commonly fatal result of inadequate bowel perfusion that requires immediate evaluation by both vascular and general surgeons. Treatment often involves vascular repair as well as bowel resection and the possible need for parenteral nutrition. Little data exist regarding the rates of bowel resection following endovascular vs open repair of AMI.
CONCLUSIONS: Endovascular intervention for AMI had increased significantly in the modern era. Among AMI patients undergoing revascularization, endovascular treatment was associated with decreased mortality and shorter length of stay. Furthermore, endovascular intervention was associated with lower rates of bowel resection and need for TPN. Further research is warranted to determine if increased use of endovascular repair could improve overall and gastrointestinal outcomes among patients requiring vascular repair for AMI.
Comparison of open and endovascular treatment of acute mesenteric ischemia.
Beaulieu RJ, Arnaoutakis KD, Abularrage CJ, Efron DT, Schneider E, Black JH 3rd.
J Vasc Surg. 2014 Jan;59(1):159-64.
CONCLUSIONS: Endovascular intervention for AMI had increased significantly in the modern era. Among AMI patients undergoing revascularization, endovascular treatment was associated with decreased mortality and shorter length of stay. Furthermore, endovascular intervention was associated with lower rates of bowel resection and need for TPN. Further research is warranted to determine if increased use of endovascular repair could improve overall and gastrointestinal outcomes among patients requiring vascular repair for AMI.
Comparison of open and endovascular treatment of acute mesenteric ischemia.
Beaulieu RJ, Arnaoutakis KD, Abularrage CJ, Efron DT, Schneider E, Black JH 3rd.
J Vasc Surg. 2014 Jan;59(1):159-64.
Bowel and Mesenteric Trauma: facts
- Less than 5% of patients with severe abdominal trauma have bowel injuries
- Delays in diagnosis as short as 8-12 hours increase the rate of morbidity and mortality from peritonitis and sepsis
- Small bowel is involved in over 50% of cases and proximal jejunum and distal ileum most commonly involved
Bowel and Mesenteric Trauma: CT Findings
- Transection of the bowel wall with focal discontinuity
- Extraluminal oral contrast material
- Pneumoperitoneum
- Hematoma in bowel wall or mesentery
- Peritoneal extravasation of intravenous contrast enhanced blood
- Bowel wall thickening with or without abnormal enhancement
Pneumoperitoneum: Causes Beyond Bowel Perforation
- Intraperitoneal rupture of the bladder with foley catheter
- Massive pneumothorax
- Barotrauma
- Peritoneal lavage
- Benign pneumoperitoneum
Small Bowel Wall Trauma: Facts
- Focal bowel wall thickening especially when associated with fluid in adjacent mesentery is an important finding of trauma
- Diffuse bowel wall thickening may be due to the hypoperfusion complex (shock bowel)
- Mesenteric injuries can occur without bowel injury and can include active bleeding or injury to the mesenteric vessels
“ Multidetector CT technology offers unprecented imaging capabilities that can be readily applied for optimal evaluation of the polytrauma patient.”
Multidetector CT of Blunt Abdominal Trauma: State of the Art
Soto JA, Anderson SW
Radiology 2012;265:678-693
“ However, to maximize the diagnostic potential of the examination and, at the same time, minimize risks, CT protocols need to be tailored to match the need of each individual patient.”
Multidetector CT of Blunt Abdominal Trauma: State of the Art
Soto JA, Anderson SW
Radiology 2012;265:678-693
Celiac and SMA Dissection: Facts
-Usually isolated finding but both vessels can be involved in up to 10% of cases
-Clinical presentation is persistent abdominal pain but most cases are incidental findings
-Treatment may be conservative (anticoagulation, analgesics and beta blockade)
-Intervention may be necessary with persistent symptoms, expansion of the false lumen or true lumen compromise
Splenic Artery Aneurysms: Etiologies
-Atherosclerosis
-Portal hypertension
-Hepatic transplant
-Pregnancy
-Collagen vascular disease
-Cirrhosis
Mesenteric Artery Aneurysms: Facts
-Most common artery is splenic artery (60%)
-Hepatic artery, SMA, celiac are the other common location in sequential order
SMA Thrombosis: Facts
-SMA occlusion results in acute intestinal ischemia and infarction
-May be a result of thrombus from cardiac thrombus (50%), atrial fibrillation (40%)
-When acute thrombus usually in more distal portion of the SMA than proximal
Celiac and SMA Stenosis: Etiology
-Atherosclerosis (older patients)
-Median arcuate ligament syndrome (younger patients)
-Tumor encasement (pancreatic cancer)
-Pancreatitis
CT Angiography: Mesenteric Artery Evaluation: Protocols
-Phases required depend on the application with two phases usually necessary
-Contrast injection rate is 4-5 cc/sec with contrast volumes in the 80-120 cc volume range
-Contrast used is Omnipaque-350 or Visipaque-320 depending on the patients creatinine or GFR levels
-Arterial phase imaging is usually with a 25-30 second delay and nephrographic phase is at 55-60 seconds
CT Angiography: Mesenteric Artery Evaluation
-Stenosis
-Median arcuate ligament syndrome
-Thrombus
-Aneurysm
-Pseudoaneurysm
-Dissection



 Tweet
Tweet