Imaging Pearls ❯ Cardiac ❯ Coronary Artery Evaluation with Calcium Scoring
|
-- OR -- |
|
- “Additionally, nearly all young persons (men age <50 years and women age <60 years) who do not smoke or have diabetes have a low 10-year risk for ASCVD based on traditional risk factors. However, there is increasing awareness of the utility for CAC scoring in this age group and of the importance of reporting the presence of any CAC given the high lifetime risk for ASCVD.”
Incidental Coronary Artery Calcium: Nothing Is More Expensive Than a Missed Opportunity.
Blumenthal RS, Grant J, Whelton SP.
J Am Coll Cardiol. 2023 Sep 19;82(12):1203-1205. - However, this study demonstrates that by using artificial intelligence deep learning algorithms, we can easily quantify and measure CAC from noncardiac CT chest scans without any additional monetary or radiation-related cost to the patient. These results highlight the underutilization of this “free” information and demonstrate a real-world, high-impact use for AI algorithms that is ready right now to directly improve patient care. The pragmatic use of this AI algorithm and increased uptake for reporting of incidental CAC has the potential to transform the appropriate allocation of primary prevention medications, motivate asymptomatic adults to make sustained lifestyle improvements, reduce the burden of ASCVD, and potentially reverse the recent trend of increased ASCVD in the United States.
Incidental Coronary Artery Calcium: Nothing Is More Expensive Than a Missed Opportunity.
Blumenthal RS, Grant J, Whelton SP.
J Am Coll Cardiol. 2023 Sep 19;82(12):1203-1205. - Background: Coronary artery calcium (CAC) has prognostic value for major adverse cardiovascular events (MACE) in asymptomatic individuals, whereas its role in symptomatic patients is less clear.
Purpose: To assess the prognostic value of CAC scoring for MACE in participants with stable chest pain initially referred for invasive coronary angiography (ICA).
Conclusion: In participants with stable chest pain initially referred for ICA, a CAC score of 0 showed very low risk of MACE, and higher CAC scores showed increasing risk of obstructive CAD, revascularization, and MACE at follow-up.
Coronary Artery Calcium Score Predicts Major Adverse Cardiovascular Events in Stable Chest Pain
The DISCHARGE Trial Group
Radiology 2024; 310(3):e231557 - Purpose: To assess the prognostic value of CAC scoring for MACE in participants with stable chest pain initially referred for invasive coronary angiography (ICA).
Materials and Methods: This prespecified subgroup analysis from the Diagnostic Imaging Strategies for Patients With Stable Chest Pain and Intermediate Risk of Coronary Artery Disease (DISCHARGE) trial, conducted between October 2015 and April 2019 across 26 centers in 16 countries, focused on adult patients with stable chest pain referred for ICA. Participants were randomly assigned to undergo either ICA or coronary CT. CAC scores from noncontrast CT scans were categorized into low, intermediate, and high groups based on scores of 0, 1–399, and 400 or higher, respectively. The end point of the study was the occurrence of MACE (myocardial infarction, stroke, and cardiovascular death) over a median 3.5-year follow-up, analyzed using Cox proportional hazard regression tests
Coronary Artery Calcium Score Predicts Major Adverse Cardiovascular Events in Stable Chest Pain
The DISCHARGE Trial Group
Radiology 2024; 310(3):e231557 - Key Results
■ In a prospective study of 1749 participants with stable chest pain followed up for 3.5 years, those with a coronary artery calcium (CAC) score of 0 at CT had a lower prevalence of obstructive coronary artery disease (4.1%) than participants with a CAC score of 400 or higher (76.1%; P < .001).
■ The major adverse cardiovascular events rate was lower in participants with a CAC score of 0 (0.5%; hazard ratio [HR], 0.08) than a CAC score of 400 or higher (6.8%; HR, 1 [reference]; P < .001).
Coronary Artery Calcium Score Predicts Major Adverse Cardiovascular Events in Stable Chest Pain
The DISCHARGE Trial Group
Radiology 2024; 310(3):e231557 - “In conclusion, in participants with stable chest pain referred for invasive coronary angiography, a coronary artery calcium score of 0 showed very low risk of major adverse cardiovascular events (MACE) at follow-up, and increasing scores were associated with increasing rates of obstructive coronary artery disease, revascularization, and MACE.”
Coronary Artery Calcium Score Predicts Major Adverse Cardiovascular Events in Stable Chest Pain
The DISCHARGE Trial Group
Radiology 2024; 310(3):e231557
- “Although the benefits of finding an unrecognized disease early in its course seem intuitive, screening tests and the clinical decisions based on them require testing with randomized clinical trials (RCTs) to understand the magnitude of benefit (if any) and the potential for harms including radiation, psychological stress, and unnecessary downstream testing and treatment with additional costs and potential complications. Coronary artery calcium scanning (CACS), a screening test introduced in 1990 to reduce mortality from coronary artery disease (CAD), has never been evaluated in an RCT designed and powered to assess its effect on CAD or all-cause mortality.”
Coronary Artery Calcium Screening-Data First.
Garg PK, Brown DL.
JAMA Intern Med. 2023 Sep 25. doi: 10.1001/jamainternmed.2023.3250. Epub ahead of print - “Fortunately, 4 decades after the introduction of CACS, 2RCTs are underway to assess its effect on hard outcomes. Both trials are testing whether a treatment strategy based on CACS compared with calculated risk estimates results in better outcomes. The ROBINSCA (Risk Or Benefit in Screening for Cardiovascular disease) trial enrolled 43 447 people in the Netherlands beginning in 2014 and is due to conclude soon. Primary end points are coronary disease morbidity and mortality after 5 years. CorCal (Effectiveness of a Proactive Cardiovascular Primary Prevention Strategy, With or Without the Use of Coronary Calcium Screening, in Preventing Future Major Adverse Cardiac Events) will include 9000 patients in the US and is expected to conclude in 2024.Primary end points are all-cause mortality,myocardial infarction, stroke, and revascularization after 5 years. Until the results of these trials become available, we caution against routine clinical CAC screening and agree with Tattersall et al that the appropriate response to the incidental discovery of coronary calcium should be to discuss vascular risk generally without provoking unnecessary anxiety, automatic referrals to specialists, inappropriate testing in absence of symptoms, or initiation of statin or aspirin therapy.”
Coronary Artery Calcium Screening-Data First.
Garg PK, Brown DL.
JAMA Intern Med. 2023 Sep 25. doi: 10.1001/jamainternmed.2023.3250. Epub ahead of print - “Incidental pertinent reportable cardiac findings are common on abdominal CTs and are frequently not reported by radiologists. These findings are of clinical relevance since patients with pertinent reportable cardiac findings have a significantly higher incidence of cardiovascular events on follow-up.”
Abdominopelvic Computed Tomography: Prevalence and Association with Subsequent Cardiovascular Events Meyersohn, NM et al.
Acad Radiol 2023; 30:2514–2520 - “Eighty-five of 222 (38.3%) patients (52.7% females, median age 52.5 years) had at least one pertinent reportable cardiac finding on the abdominopelvic CT, with a total of 140 findings in this group. From the total 140 findings, 100 (71.4%) were not reported. The most common findings seen on abdominal CTs were: coronary artery calcification (66 patients), heart or chamber enlargement (25), valve abnormality (19), sternotomy and surgery signs (9), LV wall thickening (7), device (5), LV wall thinning (2), pericardial effusion (5), and others (3). After a mean follow-up of 43.9 months, 19 cardiovascular events were found in the cohort (transient ischemic attack, cerebrovascular accident, myocardial infarction, cardiac arrest, acute arrhythmia, palpitation, syncope and acute chest pain). Only 1 event occurred in the group of patients with no incidental pertinent reportable cardiac findings (1/137 = 0.73%).”
Abdominopelvic Computed Tomography: Prevalence and Association with Subsequent Cardiovascular Events Meyersohn, NM et al.
Acad Radiol 2023; 30:2514–2520 - “Our study demonstrated a high prevalence of pertinent reportable cardiac findings in patients undergoing abdominopelvic CT for abdominal pain (38.3%). Moreover, in the group of patients with at least one cardiac finding, cardiovascular events on follow-up were significantly more common. It should be noted that the mean age of the group of patients with at least one cardiac finding was significantly higher than the group of patients without findings (75.4 yo vs 50.7 yo, p < 0.001), consistent with the established association of increasing age and risk factors for cardiovascular events. Our review also suggests that cardiac findings are often overlooked on abdominal CTs, even when performed for evaluation of upper abdominal pain in which cardiovascular disease is apotential differential diagnosis.”
Abdominopelvic Computed Tomography: Prevalence and Association with Subsequent Cardiovascular Events Meyersohn, NM et al.
Acad Radiol 2023; 30:2514–2520 - In conclusion, recognition of pertinent reportable incident cardiac findings such as coronary artery disease, valvular abnormalities, and chamber enlargement is possible on abdominopelvic CT, however many of these findings are not detected or not included in CT reports. Given that cardiovascular disease remains the leading cause of mortality in the United States in men and women, radiologists who interpret abdominopelvic CT should strive to identify and report these findings, especially as they may be the first to detect them. These findings have real clinical significance as our review suggests that patients with cardiac findings have a higher incidence of cardiovascular events on follow-up, and may be candidates for early detection and medical or surgical management. Given that the majority of pertinent reportable cardiac findings were not described in the original report, increased focus by radiologists on cardiac pathologies in the review and interpretation of abdominopelvic CT examinations presents a meaningful opportunity to impact patient care.
Abdominopelvic Computed Tomography: Prevalence and Association with Subsequent Cardiovascular Events Meyersohn, NM et al.
Acad Radiol 2023; 30:2514–2520
- IMPORTANCE Coronary artery calcium scores (CACS) are used to help assess patients’ cardiovascular status and risk. However, their best use in risk assessment beyond traditional cardiovascular factors in primary prevention is uncertain.
CONCLUSIONS AND RELEVANCE This systematic review and meta-analysis found that the CACS appears to add some further discrimination to the traditional CVD risk assessment equations used in these studies, which appears to be relatively consistent across studies. However, the modest gain may often be outweighed by costs, rates of incidental findings, and radiation risks. Although the CACS may have a role for refining risk assessment in selected patients, which patients would benefit remains unclear. At present, no evidence suggests that adding CACS to traditional risk scores provides clinical benefit.
Evaluation of the Incremental Value of a Coronary Artery Calcium Score Beyond Traditional Cardiovascular Risk Assessment A Systematic Review and Meta-analysis
Katy J. L. Bell et al.
JAMA Intern Med. 2022;182(6):634-642. - Key Points
Question: Is there an incremental gain from the addition of a coronary artery calcium score (CACS) to a standard cardiovascular disease (CVD) risk calculator?
Findings: In this systematic review and meta-analysis, the pooled gain in C statistics from adding CACS was 0.036. Most participants reclassified as being at intermediate or high risk by CACS did not have a CVD event during follow-up (range, 5.1 to 10.0 years).
Meaning: Although CACS appears to add some further discrimination to standard CVD risk calculators, no evidence suggests that this provides clinical benefit.
Evaluation of the Incremental Value of a Coronary Artery Calcium Score Beyond Traditional Cardiovascular Risk Assessment A Systematic Review and Meta-analysis
Katy J. L. Bell et al.
JAMA Intern Med. 2022;182(6):634-642. - “This systematic review and meta-analysis suggests that the CACS adds further discrimination to the traditional CVD risk assessment equations used in these studies, and the effect appears relatively consistent across studies. However, the modest gain may often be outweighed by costs, rates of incidental findings, and radiation risks. Although a CACS may have a role for refining risk assessment in selected patients, which patients would benefit remains unclear. At present, no evidence suggests that adding the CACS to traditional risk scores provides clinical benefit.”
Evaluation of the Incremental Value of a Coronary Artery Calcium Score Beyond Traditional Cardiovascular Risk Assessment A Systematic Review and Meta-analysis
Katy J. L. Bell et al.
JAMA Intern Med. 2022;182(6):634-642.
- “Coronary artery calcium is a highly specific marker for atherosclerosis and represents an integration of all the risk factors over the lifetime of an individual. Coronary artery calcium is a robust predictor of future cardiovascular events, independent of the traditional markers such as the Framingham risk score (FRS).”
Coronary Artery Calcium Scoring: Current Status and Review of Literature
Malguria N, Zimmerman S, Fishman EK
J Comput Assist Tomogr 2018;42: 887–897 - ”Agatston score is the most commonly used scoring method and defines CAC as any calcium within the coronary arterial system 130 HU or higher, occupying at least 2 to 3 adjacent pixels. The score is determined by summation of the product of the total plaque area and a cofactor determined by the maximum calcium density within the plaque; 1 for lesions with a maximum density of 130 to 199 HU, 2 for lesions with a maximum density of 200 to 299 HU, 3 for lesions with a maximum density of 300 to 399 HU, and 4 for lesions with a density of 400 HU and higher.”
Coronary Artery Calcium Scoring: Current Status and Review of Literature
Malguria N, Zimmerman S, Fishman EK
J Comput Assist Tomogr 2018;42: 887–897 - Calcium Score Calculation Errors
a. Inclusion of mitral annular calcification, mistaken as circumflex calcium, which can cause very high false calcium score
b. Mistaking aortic root calcium for coronary calcium. We exclude ostial calcium to ensure that aortic root calcium is not included in the score.
c. Motion related beam hardening artifacts may cause overestimation of score
d. Inclusion of coronary stents results in inappropriately high scores. - “The current paradigm of preventive cardiology is future cardiovascular risk prediction, which is performed using cardiovascular risk scores in asymptomatic patients with no known coronary artery disease. Based on the risk allocation, patients are prescribed statins or aspirin, with a goal toward absolute or percentage improvement in low-density lipoprotein cholesterol levels, cholesterol ratio, and systolic blood pressure.”
Coronary Artery Calcium Scoring: Current Status and Review of Literature
Malguria N, Zimmerman S, Fishman EK
J Comput Assist Tomogr 2018;42: 887–897 - “A 2017 consensus state- ment of the SCCT recommended performing CAC testing in the context of shared decision making for asymptomatic individuals aged 40 to 75 years of age without clinical ASCVD who are in the 5% to 20% 10-year ASCVD risk group (intermediate risk) and selectively in individuals who are in the less than 5% (low risk) 10-year ASCVD, such as those with a family history of pre- mature coronary artery disease.”
Coronary Artery Calcium Scoring: Current Status and Review of Literature
Malguria N, Zimmerman S, Fishman EK
J Comput Assist Tomogr 2018;42: 887–897 - The presence of calcium on routine noncontrast ungated chest CT is associated with future cardiovascular risk and is currently recommended to be reported on every NCCT, with visual scoring methods demonstrating good correlation with Agatston score categories.
Coronary Artery Calcium Scoring: Current Status and Review of Literature
Malguria N, Zimmerman S, Fishman EK
J Comput Assist Tomogr 2018;42: 887–897 - “The strong relationship between zero calcium score and very low cardiovascular event rate applies only to asymptomatic individuals. In a study of 133 symptomatic (chest pain) high-risk patients, the median CAC was 66 and 19% of patients had a negative CAC scan. Of symptomatic patients with CAC = 0, 32% patients showed a significant stenosis on invasive angiography . In this scenario other factors come into play like a much higher pre-test probability and the pathophysiological issues of plaque rupture, non- calcified plaque and thrombotic occlusions, none of which are detected by the calcium score. Therefore, a negative CAC scan cannot be used to rule out relevant obstruction in the setting of symptomatic patients.”
CT calcium scoring. History, current status and outlook
V. Sandfort, D.A. Bluemke
Diagnostic and Interventional Imaging (2017) 98, 3—10 - “The strong relationship between zero calcium score and very low cardiovascular event rate applies only to asymp- tomatic individuals. In a study of 133 symptomatic (chest pain) high-risk patients, the median CAC was 66 and 19% of patients had a negative CAC scan. Of symptomatic patients with CAC = 0, 32% patients showed a significant stenosis on invasive angiography . In this scenario other factors come into play like a much higher pre-test probability and the pathophysiological issues of plaque rupture, non- calcified plaque and thrombotic occlusions, none of which are detected by the calcium score.”
CT calcium scoring. History, current status and outlook
V. Sandfort, D.A. Bluemke
Diagnostic and Interventional Imaging (2017) 98, 3—10 - “In a study of 133 symptomatic (chest pain) high-risk patients, the median CAC was 66 and 19% of patients had a negative CAC scan. Of symptomatic patients with CAC = 0, 32% patients showed a significant stenosis on invasive angiography . In this scenario other factors come into play like a much higher pre-test probability and the pathophysiological issues of plaque rupture, non- calcified plaque and thrombotic occlusions, none of which are detected by the calcium score. Therefore, a negative CAC scan cannot be used to rule out relevant obstruction in the setting of symptomatic patients.”
CT calcium scoring. History, current status and outlook
V. Sandfort, D.A. Bluemke
Diagnostic and Interventional Imaging (2017) 98, 3—10 - “In summary, physicians need to be aware of elevated cardiac risk with higher absolute calcium scores. At the same time, a subject with low calcium score but a high percentile rank compared to his peers likely still has an elevated long term risk. This dual approach is also reflected in the 2013 ACC/AHA guidelines by specifying an absolute and a relative cutoff for CAC risk assessment (≥ 300 or ≥ 75th percentile).”
CT calcium scoring. History, current status and outlook
V. Sandfort, D.A. Bluemke
Diagnostic and Interventional Imaging (2017) 98, 3—10 - ”In summary, repeat calcium scoring in patients with a positive CAC has not been shown to help in treatment decisions. Due to the increase of CAC in relationship to age, multiple CAC scoring sessions may lead to unjustified concerns in patients and possibly unnecessary downstream testing. At this time, repeat CAC scoring is not recommended.”
CT calcium scoring. History, current status and outlook
V. Sandfort, D.A. Bluemke
Diagnostic and Interventional Imaging (2017) 98, 3—10 - ” If coronary calcium has been identified in a patient, is there any value in performing a follow-up scan to evaluate progression? Multiple prospective, randomized statin trials have evaluated repeat CAC testing. In nearly all trials, the calcium score increased over time in both treatment and placebo groups without statistical intergroup differences. Whether calcium progression is a prognostic indicator above the baseline calcium score is unclear. No clinical algorithm for treatment decisions based on calcium progression exists to date.”
CT calcium scoring. History, current status and outlook
V. Sandfort, D.A. Bluemke
Diagnostic and Interventional Imaging (2017) 98, 3—10
- “It is estimated that in 2007, over 13 million chest CT examinations were performed, with less than 1 million being electrocardiogram-gated. Since CAC is often observed on standard non-contrast chest CT examinations performed without ECG gating, there is an opportunity to use this CAC information to implement preventive management in a large number of patients not known to have coronary atherosclerosis.”
Incidental coronary calcifications on routine chest CT: Clinical implications Pakdaman MN et al. Trends in Cardiovascular Medicine , Volume 27 , Issue 7 , 475 - 480 - “Of note, a true CAC score of 0 can only be reliably determined with gated studies, as studies using routine non-gated chest CT may show 0 among patients with CAC 0–9 on gated studies. Hutt et al. used ECG-gated CT as the gold standard to investigate the reliability of non-gated CT in detecting coronary calcification. They found a sensitivity of 96.4% and specificity of 100% for the detection of CAC. A review of four studies comprising 1153 subjects found a false-negative rate of 8.3%.”
Incidental coronary calcifications on routine chest CT: Clinical implications Pakdaman MN et al. Trends in Cardiovascular Medicine , Volume 27 , Issue 7 , 475 - 480 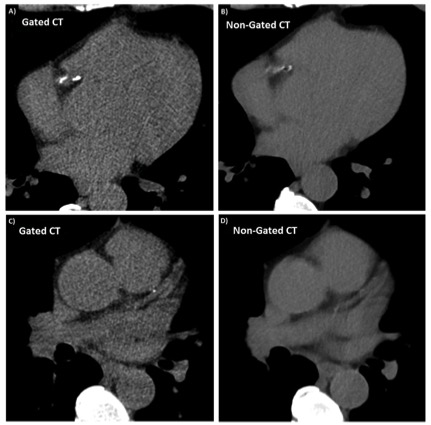
Incidental coronary calcifications on routine chest CT: Clinical implications Pakdaman MN et al. Trends in Cardiovascular Medicine , Volume 27 , Issue 7 , 475 - 480- “Unfortunately, cardiac findings are often overlooked on CT or may not be reported or adequately emphasized in the impression on the final report. Based on the high impact of incidental coronary calcifications on non-gated chest CT and the impact of CAC measurement on the management and outcome, we recommend increased attention be made to incidental coronary calcifications during the radiographic search pattern, with inclusion of positive findings in the impression of the final report.”
Incidental coronary calcifications on routine chest CT: Clinical implications Pakdaman MN et al. Trends in Cardiovascular Medicine , Volume 27 , Issue 7 , 475 - 480 - “While the reports from chest CT are likely, for at least the near future, to use the most basic of quantitative descriptors rather than scores such as the Agatston score, consideration might be given to the performance of ECG- gated CT scans in patients, unless the amount described is reported as extensive. Discussion with patients regarding preventive lifestyle modifications including a heart healthy diet and aerobic exercise programs would also be appropriate when any CAC is found.”
Incidental coronary calcifications on routine chest CT: Clinical implications Pakdaman MN et al. Trends in Cardiovascular Medicine , Volume 27 , Issue 7 , 475 - 480 - OBJECTIVES: The aim of this study was to investigate whether inclusion of simple measures of calcified plaque distribution might improve the ability of the traditional Agatston coronary artery calcium (CAC) score to predict cardiovascular events
BACKGROUND: Agatston CAC scoring does not include information on the location and distributional pattern of detectable calcified plaque.
CONCLUSIONS: The number of coronary arteries with calcified plaque, indicating increasingly “diffuse” multivessel subclinical atherosclerosis, adds significantly to the traditional Agatston CAC score for the prediction of CHD and CVD events.
Improving the CAC Score by Addition of Regional Measures of Calcium Distribution Blaha MJ et al. J Am Coll Cardiol Img 2016;9:1407–16 - “In our study of a well-defined multiethnic cohort free of baseline CVD, we have shown that measures of diffuse CAC distribution add predictive value to the Agatston CAC score, particularly when traditional CAC scores are in the intermediate range (1 to 300). This incremental predictive value is of similar magnitude to that commonly attributed to adding novel serum biomarkers to traditional risk factors in intermediate-risk patients.”
Improving the CAC Score by Addition of Regional Measures of Calcium Distribution Blaha MJ et al. J Am Coll Cardiol Img 2016;9:1407–16 - “We have shown that readily available measures of diffuse CAC distribution add to the traditional Agat- ston CAC score for the prediction of CHD and CVD events. While we await development of a new comprehensive CAC scoring algorithm, clinicians may consider reporting and interpreting the number of vessels with CAC in addition to a total CAC burden score on routine ungated and gated noncontrast chest and cardiac CT scans, particularly when CAC burden is intermediate.”
Improving the CAC Score by Addition of Regional Measures of Calcium Distribution Blaha MJ et al. J Am Coll Cardiol Img 2016;9:1407–16 - “In patients for whom the development or progression of CAC would support intensification or alteration in preventive management, it may be appropriate to consider repeat CAC scanning at an interval of 5 years for patients with 0 CAC and a 3-5 year interval for patients with >0 CAC.”
Clinical indications for coronary artery calcium scoring in asymptomatic patients: Expert consensus statement from the Society of Cardiovascular Computed Tomography Hecht h et al. Journal of Cardiovascular Computed Tomography 11(2017) , 157 - 168 - “It may be appropriate to include CAC scanning in CCTA protocols in symptomatic patients without established CAD undergoing CTA, and in high risk asymptomatic individuals for whom the CCTA appropriateness criterion is uncertain, as well as in asymptomatic patients referred for preoperative evaluation prior to major surgery.”
Clinical indications for coronary artery calcium scoring in asymptomatic patients: Expert consensus statement from the Society of Cardiovascular Computed Tomography Hecht H et al. Journal of Cardiovascular Computed Tomography 11(2017) , 157 - 168 - “Consistent with a prior guideline from the SCCT/STR, CAC scoring of noncontrast chest CT scans is appropriate in all lung cancer screening patients and patients greater than 40 years of age without established ASCVD. The presence of CAC should be noted in the report of all NCCT studies.”
Clinical indications for coronary artery calcium scoring in asymptomatic patients: Expert consensus statement from the Society of Cardiovascular Computed Tomography Hecht H et al. Journal of Cardiovascular Computed Tomography 11(2017) , 157 - 168 - CAD-RADS: Coronary Artery
Disease - Reporting and Data System.
An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Radiology (ACR) and the North American Society for Cardiovascular Imaging (NASCI). Endorsed by the American College of Cardiology
Cury RC et al. J Am Coll Radiol 2016;13:1458-1466 - The proposed reporting system for coronary artery disease is?
A. BI-RADS
B. LI-RADS
C. Lung-RADS
D. PI-RADS
E. CAD-RADS - BI-RADS (breast for screening mammography)
LI-RADS (standardization reporting in patients with chronic liver disease)
Lung-RADS (standardization reporting of high-risk smokers undergoing CT lung screening)
PI-RADS (multi-parametric MR imaging in the context of prostate cancer)
CAD-RADS (standardized reporting system for coronary CTA results on a per-patient basis.) - “The suggested CAD-RADS classification is applied on a per-patient basis and represents the highest-grade coronary artery lesion documented by coronary CTA. It ranges from CAD-RADS 0 (Zero) for the complete absence of stenosis and plaque to CAD-RADS 5 for the presence of at least one totally occluded coronary artery and should always be interpreted in conjunction with the impression found in the report.”
CAD-RADS: Coronary Artery Disease - Reporting and Data System. Cury RC et al. J Am Coll Radiol 2016;13:1458-1466 - “The main goal of CAD-RADS is to standardize reporting of coronary CTA results and to facilitate communication of test results to referring physicians along with suggestions for subsequent patient management. In addition, CAD-RADS will provide a framework of standardization that may benefit education, research, peer-review and quality assurance with the potential to ultimately result in improved quality of care.”
CAD-RADS: Coronary Artery Disease - Reporting and Data System. Cury RC et al. J Am Coll Radiol 2016;13:1458-1466

- “As coronary artery calcification (CAC) represents direct evidence of coronary atherosclerosis with excellent negative predictive values in patients without presence of CAC, it suggests itself to be beneficial for risk stratification of patients with suspected ACS and potentially advantageous as opposed to clinical risk scores alone. In fact, in this low-intermediate risk population only 10% of patient.”
Identification of coronary artery calcification can optimize risk stratification in patients with acute chest pain Bittner DO et al International Journal of Cardiology 249 (2017) 473–478 - “In this large real-world clinical scenario of patients with acute chest pain, we could demonstrate a strong association of the extent of CAC to the severity of CAD and the incidence of ACS. Identification of CAC in addition to clinical risk assessment using TIMI risk score provides an excellent negative predictive value to identify patients at low risk for obstructive CAD and ACS. The clinical value of this combined effort might improve patient management in settings where more advanced imaging is not available.”
Identification of coronary artery calcification can optimize risk stratification in patients with acute chest pain Bittner DO et al International Journal of Cardiology 249 (2017) 473–478
- “Because of the complexity of coronary anatomy, the frequency of motion and calcium-related image artifacts, and the morphologic subtleties of lesions, interpreters must review coronary CTA interactively on cardiac-specific interpretation software platforms capable of 2- and 3-dimensional displays in all conventional reconstruction formats. These include transaxial 2-dimensional image stacks, multiplanar reformations (MPR), maximum intensity projections (MIP), curved multiplanar reformations (cMPR), and volume rendering technique (VRT) reconstructions.” SCCT guidelines for the interpretation and reporting of coronary CT angiography: A report of the Society of Cardiovascular Computed Tomography Guidelines Committee Leipsic J et al Journal of Cardiovascular Computed Tomography 8 (2014) 342-358
- “ CACS, performed on either an electron-beam CT or MDCT, is a proven marker for the presence of coronary atherosclerosis and risk of future cardiovascular events. CACS is useful in risk stratification and reclassification, as a strong association has been found between the calcium score and future mortality and/or adverse cardiac events.” ACR Appropriateness Criteria Asymptomatic Patient at Risk for Coronary Artery Disease Earls JP et al. J Am Coll Radiol 2014;11:12-19.
- “The coronary artery calcium score (CACS) is a marker of vascular injury that correlates closely with the overall atherosclerotic burden. Individual data derived from this and other imaging tests provide useful prognostic information for patient management and can complement current risk prediction models.” ACR Appropriateness Criteria Asymptomatic Patient at Risk for Coronary Artery Disease Earls JP et al. J Am Coll Radiol 2014;11:12-19.
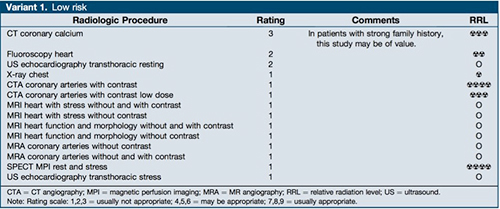
- “In low-risk patients (See Variant 1), all modalities were considered “usually not appropriate,” but the panel did comment that CACS may be useful in low-risk patients who have a strong family history of coronary risk.” ACR Appropriateness Criteria Asymptomatic Patient at Risk for Coronary Artery Disease Earls JP et al. J Am Coll Radiol 2014;11:12-19.
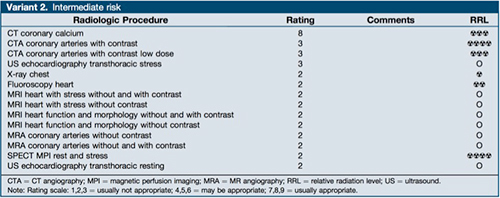
- “In intermediate-risk patients (See Variant 2), CACS was determined to be “usually appropriate,” as it can be used to stratify and reclassify patient risk more accurately than traditional methods.” ACR Appropriateness Criteria Asymptomatic Patient at Risk for Coronary Artery Disease Earls JP et al. J Am Coll Radiol 2014;11:12-19.
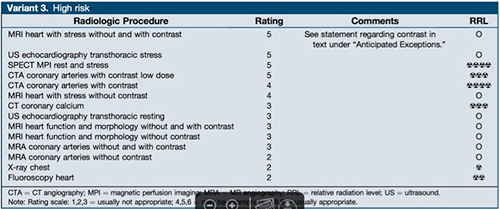
- “In high-risk patients (See Variant 3), it was determined that CCTA and stress-and-rest studies using MRI, single-photon emission CT, MPI, and ultrasound “may be appropriate.” ACR Appropriateness Criteria Asymptomatic Patient at Risk for Coronary Artery Disease Earls JP et al. J Am Coll Radiol 2014;11:12-19.
- Intermediate Risk Patient
- Low Risk Patient
- High Risk Patient



- “ Increasing calcified plaque in coronary arteries continues to predict a graded decrease in survival among patients with extensive Agatston score > 1000 with no apparent upper threshold.”
All-cause mortality in asymptomatic persons with extensive Agatston scores above 1000
Patel J et al.
J Cardiovasc Comput Tomogr 8 (2014) 26-32 - “ After multivariable adjustment, Agatston scores 1001 to 1500, Agatston score 1501 to 2000 and >2000 were associated with an 8.05, 7.45, and 13.26 fold greater mortality risk, respectively, than for Agatston score of 0 .”
All-cause mortality in asymptomatic persons with extensive Agatston scores above 1000
Patel J et al.
J Cardiovasc Comput Tomogr 8 (2014) 26-32 - “ The phenotype of Agatston score >1000 represents a distinct advance form of atherosclerosis with a greater all-cause mortality risk than Agatston score < 1000. Agatston score >2000 portends a nearly 2 fold higher mortality risk than Agatston score 1001 to 1500.”
All-cause mortality in asymptomatic persons with extensive Agatston scores above 1000
Patel J et al.
J Cardiovasc Comput Tomogr 8 (2014) 26-32
- “ In this observational study, coronary artery calcification (CAC) on noncardiac chest CT (NCCT) in this enriched population was often unreported. Although NCCT can indicate presence and location of CAC, these features are rarely reported, even when involving locations such as the left main coronary artery or the left anterior descending coronary artery. In view of its diagnostic and prognostic importance, evaluation of CAC should become a routine part of interpretation of NCCT.”
Frequency of unrecognized, unreported, or undereported coronary artery and cardiovascular calcification on noncardiac chest CT
Williams KA et al
J Cardiovasc Comput Tomogr 7 (2013) 167-172 - “ Although NCCT can indicate presence and location of CAC, these features are rarely reported, even when involving locations such as the left main coronary artery or the left anterior descending coronary artery. In view of its diagnostic and prognostic importance, evaluation of CAC should become a routine part of interpretation of NCCT.”
Frequency of unrecognized, unreported, or undereported coronary artery and cardiovascular calcification on noncardiac chest CT
Williams KA et al
J Cardiovasc Comput Tomogr 7 (2013) 167-172 - “CAC was present in 207 of the 355 patients (58% of the group) but was recorded in the final radiology report as present in only 44% of these subjects. CAC in the left main coronary artery was evident on review in 139 patients but was specified in the final report in only 1 patient. Left anterior descending CAC was evident in 188 patients but reported in only 3%.”
Frequency of unrecognized, unreported, or undereported coronary artery and cardiovascular calcification on noncardiac chest CT
Williams KA et al
J Cardiovasc Comput Tomogr 7 (2013) 167-172 - “This study shows that underreporting of cardiovascular calcification on NCCTs of the thorax is frequent. Because the finding of vascular or valvular calcification would have clinical significance and potentially can result in a change in treatment and patient behavior, recognition and reporting of these findings should become routine during interpretation of NCCTs.”
Frequency of unrecognized, unreported, or undereported coronary artery and cardiovascular calcification on noncardiac chest CT
Williams KA et al
J Cardiovasc Comput Tomogr 7 (2013) 167-172
- “ Coronary calcium was found only in men >34 years of age. Of the 53% who had positive scans (Agaston score >0), 87% had higher than average Agaston scores compared with a national database. Agaston score above the 75th percentile was found in 57% of firefighters. No correlation was observed between traditional risk factors and those with and without coronary calcium.”
Coronary calcium scoring independently detects coronary artery disease in asymptomatic firefighters: A prospective study
Santora LJ et al.
J Cardiovasc Comput Tomogr 7 (2013) 46-50 - “The majority of coronary plaque was noncalcified, particularly in younger
individuals. Conditioning aggressive primary prevention on traditional CCP scoring algorithms may obviate appropriate risk reduction interventions in younger persons with
a family history of early-onset CAD.”
Noncalcified Coronary Plaque Volumes in Healthy People with a Family History of
Early-Onset Coronary Artery Disease
Kral B et al
JACC (submitted) - Noncalcified Coronary Plaque Volumes in Healthy People with a Family History of
Early-Onset Coronary Artery Disease
Brian G. Kral, M.D., M.P.H. Diane M. Becker, Sc.D., M.P.H., Dhananjay Vaidya,
M.B.B.S., Ph.D., Lisa R. Yanek, M.P.H., Rehan Qayyum, M.D., M.H.S., Stefan L.
Zimmerman, M.D.,† Damini Dey, Ph.D., Taryn F. Moy, M.S., Elliot K. Fishman,
M.D.,† Lewis C. Becker, M.D.
JACC (submitted) - “ Coronary artery calcium can be detected on CTA images with high accuracy. The Agatston calcium score derived from CT images shows good correlation with unenhanced CT calcium score and is highly reproducible. However, higher Agatston scores are systematically underestimated when derived from CTA images.”
Assessment of Agatston Coronary Calcium Score Using Contrast Enhanced CT Coronary Angiography
va der Bijl N et al.
AJR 2010;195:1299-1305
- “ While mere numeric values might be different, commercially available software platforms produce comparable CAC scoring results, which suggests a vendor-independence of the method; however, none of the analyzed software platforms appears to provide a distinct advantage for risk stratification, as the variability of CAC scores depending on the reconstruction interval persists across platforms.”
Interplatform Reproducibility of CT Coronary Calcium Scoring Software
Weininger M et al.
Radiology 2012;265:70-77 - “ Vendor independent reproducibiity of coronary artery calcium scores is a prerequisite for reliable comparison of results and has direct impact on cardiovascular risk stratification, risk modification, and therapeutic monitoring.”
Interplatform Reproducibility of CT Coronary Calcium Scoring Software
Weininger M et al.
Radiology 2012;265:70-77 - “ Within our population, Spearman rank correlation between the workstations was highest at 60% of the R-R interval, which supports the clinical use of this time point during the cardiac cycle for image reconstruction at CT CAC scoring.”
Interplatform Reproducibility of CT Coronary Calcium Scoring Software
Weininger M et al.
Radiology 2012;265:70-77 - Workstation Platforms Used in Comparison
- Syngo Calcium Scoring ( Siemens Healthcare)
- Aquarius (TeraRecon Inc)
- Vitrea (Vital Images)
- “ The acquisition of a coronary calcium score in every symptomatic patient referred for coronary CT angiography requires a case by case approach.”
Coronary Calcium Scan Acquisition Before Coronary CT Angiography: Limited Benefit or Useful Addition
Torres FS et al.
AJR 2013; 200:66-73 - “ Coronary artery calcium (CAC) score may be used as a gatekeeper for coronary CT angiography (CTA) when CAC score is very high, although there is no established upper limit of the total CAC score that could be used as a threshold above which coronary CTA should not be performed.”
CT Perfusion in Oncologic Imaging: A Useful Tool-
Garcia-Figueiras R et al
AJR 2013; 200:8-19 - “ The absence of coronary calcification is associated with a low prevalance of obstructive coronary artery disease (CAD) and with a very good near term prognosis in symptomatic patients, with a low to intermediate pretest probability of CAD. In these patients additional information (symptoms, clinical risk factors, and results of prior tests) should be entertained when considering deferring the coronary CTA on the basis of a CAC score of zero.”
CT Perfusion in Oncologic Imaging: A Useful Tool-
Garcia-Figueiras R et al
AJR 2013; 200:8-19 - “ Radiation dose from a CAC score and coronary CTA may vary widely. Newer scanner technologies and the use of radiation dose reduction strategies have helped to significantly decrease the radiation dose in both tests. If CAC score is to be acquired, much attention should be put to minimize radiation exposure and to plan the scanning range of the coronary CTA on the basis of coronary calcium score images.”
CT Perfusion in Oncologic Imaging: A Useful Tool-
Garcia-Figueiras R et al
AJR 2013; 200:8-19
- “ Budoff et al, in the Multi-Ethnic study of Atherosclerosis (MESA), has shown that even minimal CAC (Agaston scores of 1-10) increased the risk of CHD 3-fold and a score >100 confers a 10-fold risk of future cardiovascular events.”
Risk stratification of non-contrast CT beyond the coronary calcium scan
Madaj P, Budoff MJ
J Cardiovasc Comput Tomogr (2012) 6, 301-307 - “ The investigators concluded that patients with frequent lesions in the left main or patients with a higher number of calcified lesions have a significantly higher risk of mortality. The clincal implications are simple,clinicians can also report lesion counts in addition to total Agaston score, noting that larger number of lesions imparts a higher clinical significance.”
Risk stratification of non-contrast CT beyond the coronary calcium scan
Madaj P, Budoff MJ
J Cardiovasc Comput Tomogr (2012) 6, 301-307
- “ Coronary artery calcium (CAC) is an independent predictor of coronary artery disease (CAD) events and improves the ability to predict risk in vulnerable groups, adding information beyond current global risk assessment methods.”
Role of Nonenhanced Multidetector CT Coronary Artery Calcium Testing in Asymptomatic and Symptomatic Individuals
Nasir K, Clouse M
Radiology 2012; 264:637-649 - “ A zero coronary calcium score stands as perhaps the most powerful negative risk factor for development of a coronary event.”
Role of Nonenhanced Multidetector CT Coronary Artery Calcium Testing in Asymptomatic and Symptomatic Individuals
Nasir K, Clouse M
Radiology 2012; 264:637-649 - “ Emerging data suggest there are individuals considered to be in the low risk group who may benefit from CAC screening, especially those with a family history of premature CAD and woman younger than 60 years: further studies are needed for both groups.”
Role of Nonenhanced Multidetector CT Coronary Artery Calcium Testing in Asymptomatic and Symptomatic Individuals
Nasir K, Clouse M
Radiology 2012; 264:637-649 - “ CAC testing has value in triaging low and intermediate risk patients with chest pain, a role acknowledged by current guidelines as it is associated with a very low risk of future cardiac events and thus the potential to reduce downstream testing and costs.”
Role of Nonenhanced Multidetector CT Coronary Artery Calcium Testing in Asymptomatic and Symptomatic Individuals
Nasir K, Clouse M
Radiology 2012; 264:637-649 - “ It is estimated that in the next 15 years, 25 million people will die of stroke or heart disease with 80% of this burden occurring in developing countries. In approximately one-half of the individuals, the initial presentation of CAD is either myocardial infarction or sudden death.”
Role of Nonenhanced Multidetector CT Coronary Artery Calcium Testing in Asymptomatic and Symptomatic Individuals
Nasir K, Clouse M
Radiology 2012; 264:637-649 - “ Unfortunately conventional risk factor assessment can be used to predict 65-80% of future cardiovascular events, leaving many middle aged and older individuals to experience a major cardiovascular event despite being classified as low risk by means of traditional approaches.”
Role of Nonenhanced Multidetector CT Coronary Artery Calcium Testing in Asymptomatic and Symptomatic Individuals
Nasir K, Clouse M
Radiology 2012; 264:637-649 - “ These data reinforce our assessment than when CAC is used as a gatekeeper for downstream advanced testing in symptomatic individuals, pretest likelihood of CAD should always be taken into account. Absence of CAC has great potential in reducing downstream cost if used in low to intermediate risk asymptomatic individuals.”
Role of Nonenhanced Multidetector CT Coronary Artery Calcium Testing in Asymptomatic and Symptomatic Individuals
Nasir K, Clouse M
Radiology 2012; 264:637-649 - “ The National Institute for Health and Clinical Excellence clinical guidelines have also acknowledged the role of CAC in layered testing among patients presenting with chest pain.”
Role of Nonenhanced Multidetector CT Coronary Artery Calcium Testing in Asymptomatic and Symptomatic Individuals
Nasir K, Clouse M
Radiology 2012; 264:637-649
- “ We feel that the widespread use of calcium scoring in symptomatic patients is severely limited because of test imprecision and the need for additional testing in most patients.”
Calcium scoring and chest pain: Is it dead on arrival
Villines TC et al.
J Cardiovascular Comput Tomogr (2011) 5, 30-34 - “ Iterative reconstruction reduces image noise and blooming artifacts from calcification, leading to improved diagnostic accuracy of coronary CT angiography in patients with heavily calcified vessels.”
Evaluation of Heavily Calcified Vessels with
Coronary CT Angiography: Comparison of Iterative and Filtered Back Projection Image Reconstruction
Renker M et al.
Radiology 2011; 260:390-399
"Absolute CAC is superior to percentile rank calculated based on the MESA database in the prediction of obstructive CAD. Therefore, while for risk stratification purposes percentile rank remains an important predictor, for the purposes of predicting obstructive CAD and for further diagnostic referral, the absolute CAC might be preferred."
Absolute Coronary Artery Calcium Scores are superior to MESA percentile rank in predicting obstructive coronary artery disease
Akram K, Voros S
Int J Cardiovasc Imaging (2008) 24:743-749- " The coronary artery calcium (CAC) score above which it is recommended that coronary computerized tomographic angiography (CTA) not be performed has been steadily increasing. Currently, calcium scores > 1000 are thought to prohibit CTA accurate interpretation. However, a reasoned approach suggests that there is no absolute upper limit that applies to all patients and imaging centers."
How much calcium is too much calcium for coronary computerized tomographic angiography?
Hecht HS, Bhatti T
J Cardiovasc Comput Tomogr (2008) 2, 183-187
- " A CAC score of >1000 or a pattern of isolated large, dense calcifications with CAC < 1000 should alert personnel to potential interpretation problems and should not be followed by CTA if the interpreting physician does not have extensive experience in dealing with these issues.
How much calcium is too much calcium for coronary computerized tomographic angiography?
Hecht HS, Bhatti T
J Cardiovasc Comput Tomogr (2008) 2, 183-187
- " CCS (calcium coverage score) may enable better stratification of patients according to risk compared with the Agaston or mass score and thereby aid physicians in determining appropriate individual treatment strategies."
Coronary Calcium Coverage Score: Determination, Correlates, and Predictive Accuracy in the Multiethnic Study of Atherosclerosis
Brown ER et al.
Radiology 2008; 247:669-678
- " The calcium coverage score (CCS) was highly associated with coronary heart disease (CHD) events, and a twofold increase in CCS was associated with a 34% increase in the risk of any hard CHD event and a 52% increase in the risk of any CHD event."
Coronary Calcium Coverage Score: Determination, Correlates, and Predictive Accuracy in the Multiethnic Study of Atherosclerosis
Brown ER et al.
Radiology 2008; 247:669-678
- "Retten et al. have demonstrated that an important factor affecting measurement variability is the partial volume effect that operates when contiguous, rather than overlapping, scans are reconstructed. The practical implication of this error might be a false negative study or inaccurate categorization of the severity of patient risk."
Science to Practice: What is the Value of measuring Coronary Artery Calcification?
Wexler L
Radiology 246:1, Jan 2008;1-2
- "These large observational cohorts show that the absence of coronary artery calcification by Cardiac CT is associated with a low adverse risk and therefore could be used as a tool to counsel patients about the risk of such events."
Prognostic Significance of Zero Coronary Calcium Scores on Cardiac Computed Tomography
Shareghi S et al.
J Cardiovasc Comput Tomogr (2007)1, 155-159
- "Summary data show that in a total follow-up of 35,765 asymptomatic patients, 16,106 (45%) had scores of zero. Pooled sensitivity for CAC to detect a cardiovascular event was 98.1%, and negative predictive value was 99.9%."
Prognostic Significance of Zero Coronary Calcium Scores on Cardiac Computed Tomography
Shareghi S et al.
J Cardiovasc Comput Tomogr (2007)1, 155-159
- "In conclusion, asymptomatic persons without CAC (scores of zero) are shown to have a very low risk (0.27% per year) of future cardiovascular events during the subsequent 3-5 years and is a group unlikely to derive short term benefit from risk reducing pharmacotherapy."
Prognostic Significance of Zero Coronary Calcium Scores on Cardiac Computed Tomography
Shareghi S et al.
J Cardiovasc Comput Tomogr (2007)1, 155-159
- "Aortic calcification scores at CT colonography are significantly associated with established cardiac-related events. This screening information can be obtained without additional scanning or risk to the patient."
Assessment of Cardiovascular Risk Status at CT Colonography
Davila JA et al.
Radiology 2006; 240:110-115.
- " CT angiography was performed in 67 patients (50 male, 17 female; mean age 60.1 +/- 10.5 years) with suspected coronary artery disease and compared with invasive coronary angiography. All vessels >/=1.5 mm were considered for the assessment of significant coronary artery stenosis (diameter reduction >50%). Forty-seven patients were identified as having significant coronary stenoses on invasive angiography with 18% (176/1005) affected segments. None of the coronary segments needed to be excluded from analysis. CT correctly identified all 20 patients having no significant stenosis on invasive angiography. Overall sensitivity for classifying stenoses was 94%, specificity was 97%, positive predictive value was 87%, and negative predictive value was 99%."
- Material and Methods: Overall sensitivity for classifying stenoses was 94%, specificity was 97%, positive predictive value was 87%, and negative predictive value was 99%."
Conclusion: Sixty-four-slice CT provides a high diagnostic accuracy in assessing coronary artery stenoses.
Accuracy of MSCT coronary angiography with 64-slice technology: first experience.
Leschka S et al. Eur Heart J. 2005 Apr 19; [Epub ahead of print
- " The currently best available spatial and temporal resolution for retrospectively ECG gated coronary multi-detector-row CT angiography is 0.4 mm and 165 ms, respectively. These acquisition parameters are already rather close to cardiac catheter. Studies so far compared non-invasive coronary CT and convention angiography for the detection of coronary artery stenoses. The most promising result reported by all authors was the high negative predictive value of the CTA."
Coronary CT angiography in symptomatic patients
Becker CR.
Eur Radiol. 2005 Feb;15 Suppl 2:B33-41
- "The most promising result reported by all authors was the high negative predictive value of the CTA."
Coronary CT angiography in symptomatic patients
Becker CR.
Eur Radiol. 2005 Feb;15 Suppl 2:B33-41
- " CT Angiography is more accurate than calcium scoring in demonstrating coronary artery stenosis. A patient calcium score of greater than or equal to 400, however, can be used to potentially identify patients with significant coronary stenoses not detected at CT angiography."
Coronary Artery Stenosis: Detection with Calcium Scoring, CT Angiography, and Both Methods Combined
Lau GT et al.
Radiology 2005; 235:415-422
- " Combining CT angiography with Calcium Scoring (over 400) improved the sensitivity of CT angiography (from 93 to s100%) in demonstrating significant coronary disease in patients."
Coronary Artery Stenosis: Detection with Calcium Scoring, CT Angiography, and Both Methods Combined
Lau GT et al.
Radiology 2005; 235:415-422
- "In a population having a low pretest likelihood of significant coronary artery disease, 16-MDCT shows a moderate to high sensitivity and a high NPV for the detection or exclusion of significant disease, but has a somewhat reduced PPV compared with conventional coronary angiography."
Clinical Value of MDCT in the Diagnosis of Coronary Artery Disease in Patients with a Low Pretest Likelihood of Significant Disease
Nikolaou K et al.
AJR 2006;186:1659-1668.
- "Although 16-MDCT appeared to overestimate diagnoses as compared with QCA, resulting in a relatively high number of false-positive diagnosis of significant coronary artery disease, this may have been a consequence either of the relatively small patient population or of false negative diagnosis on QCA."
Clinical Value of MDCT in the Diagnosis of Coronary Artery Disease in Patients with a Low Pretest Likelihood of Significant Disease
Nikolaou K et al.
AJR 2006;186:1659-1668.
- "CTA has the potential to perform cross-sectional imaging through the narrowed portion of the lumen and to measure the area of the vessel lumen versus the area of an adjacent,apparently normal segment, which are not possible using QCA."
Clinical Value of MDCT in the Diagnosis of Coronary Artery Disease in Patients with a Low Pretest Likelihood of Significant Disease
Nikolaou K et al.
AJR 2006;186:1659-1668.
- Opinion
- False positive coronary CTA is less of a practical issue that false negative coronary CTA. The lack of false negative is especially critical
- "Sensitivity, specificity, and the negative predictive value (NPV) of 64-MDCT per patient were 97%, 79%, and 96%, respectively. Per segment, 923 of 1,020 coronary artery segments were assessable (90%). For the detection of stenoses of more than 50% and more than 75% per segment, 64-MDCT showed a sensitivity of 82% and 86%, respectively. Per segment, specificity and NPV were as high as 95% and 97%, respectively."
Accuracy of 64-MDCT in the diagnosis of ischemic heart disease
Nikolaou K et al
AJR 2006 July; 187(1):111-117.
- "Significant stenosis was defined as a diameter reduction of > 50%. Of 966 segments, 884 (92%) were assessable. Compared with ICAG, the sensitivity of CTA to diagnose significant stenosis was 90%, specificity 94%, positive predictive value (PPV) 89% and negative predictive value (NPV) 95%."
Diagnostic accuracy of 64-slice computed tomography for detecting angiographically significant coronary artery stenosis in an unselected consecutive patient population: comparison with conventional invasive angiography.
Ehara M et al.
Circ J 2006 May; 70(5):564-571.
- "On 64-MDCT, 89% of coronary artery segments are assessible. Ten or more vessel segments are assessable in 94% of patients."
Coronary CT Angiography with 64-MDCT: Assessment of Vessel Visibility
Pannu HK,Jacobs JE,Lai S,Fishman EK
AJR 2006; 187:119-128.
- "In clinical routine, coronary CTA will primarily be used for risk stratification on a per patient basis. In the present study, coronary 64-MDCT showed a high diagnostic accuracy on both per patient and per segment analyses."
Accuracy of 64-MDCT in the Diagnosis of Ischemic Heart Disease
Nikolaou K et al.
AJR 2006; 187:111-117.
- "In conclusion, 64 MDCT coronary angiography provides a significantly increased spatial and temporal resolution compared with earlier MDCT systems. In a clinical setting, this technique may hold great promise for the reliable diagnosis or exclusion of significant CAD on a per patient basis and could give CTA an important role in the stratification of patients with both known and suspected CAD."
Accuracy of 64-MDCT in the Diagnosis of Ischemic Heart Disease
Nikolaou K et al.
AJR 2006; 187:111-117.
- "68 of 72 coronary CT angiograms (94%) were of diagnostic image quality. QCA showed significant CAD (i.e. one or more stenosis in >50%) in 57% (39/68) and nonsignificant disease or healthy CTA’s in 43% (29/68) of the patients. Sensitivity, specificity and the negative predictive value of 64 MDCT per patient were 97%, 79%, and 96% respectively."
Accuracy of 64-MDCT in the Diagnosis of Ischemic Heart Disease
Nikolaou K et al.
AJR 2006; 187:111-117.
- Plaque Attenuation Scoring
- Predominantly lipid rich plaques; < 60HU
- Intermediate plaques: 61-119 HU
- Predominately calcified plaques: >120 HU
- Reliability of Differentiating Human Coronary Plaque Morphology Using
- Contrast Enhanced Multislice Spiral Computed Tomography
Schroeder S et al.
J Comput Assist Tomogr 2004;28:449-454
- " The finding may have implications for the interpretation of calcification of atherosclerotic plaque in other vascular beds."
Calcified Carotid Atherosclerotic Plaque Is Associated Less with Ischemic Symptoms Than Is Noncalcified Plaque on MIDST
Nandalur KR et al.
AJR 2005;184;295-298
- " Image attenuation values vary by scanner and participant body size, producing calcium score differences that are not due to true calcium burden disparities. Use of calibration phantoms may improve the comparability of such measurements between persons scanned with different scanners and within persons over time."
Measuring Coronary Calcium on CT images Adjusted for Attenuation Differences
Nelson JC et al.
Radiology 2005;235:404-414
- " Micro CT provides quantitative information about plaque morphology equivalent to that provided with histomorphometric analysis. Micro CT is feasible for analysis of the coronary artery wall."
Atherosclerotic Lesions at Micro CT: Feasibility for Analysis of Coronary Artery Wall in Autopsy Specimens
Langheinrich AC et al.
Radiology 2004; 231:675-681
- " The absence of detectable calcium does not reliably exclude substantial coronary disease."
Coronary Artery Stenosis: Detection with Calcium Scoring, CT Angiography, and Both Methods Combined
Lau GT et al.
Radiology 2005; 235:415-422
- " The accuracy of sequential MDCT for coronary calcium quantification is sufficient in most cases for stratification of patient risk."
Potential Clinical Impact of Variability in the Measurement of Coronary Artery Calcification with Sequential MDCT
Halliburton SS et al.
AJR 2005; 184:643-648
- "Differences in coronary artery calcium measurements using EBT and MDCT are similar to interscan differences in CAC measurements previously reported for EBT or for other MDCT scanners individually."
Concordance of Coronary Artery Calcium Estimates Between MDCT and Electron Beam Tomography Daniell AL et al. AJR 2005; 185:1542-1545
- "Electron beam and multidetector row CT scanners have equivalent reproducibility for measuring coronary artery calcium. Calcium volumes and interpolated volume scores are slightly more reproducible than Agatston scores."
Coronary Calcium Measurements: effect of CT Scanner Type and Calcium Measure on Rescan reproducibility-MESA Study Detrano RC et al. Radiology 2005; 236:477-484
- "MDCT is a promising tool for coronary calcium scoring; however, more studies are needed comparing EBCT and MDCT, especially at lower coronary artery calcium levels."
Electron beam CT versus helical CT scans for assessing coronary calcifications: Current utility and future directions
Nasir K, Budoff M, Post WS, Fishman EK, Mahesh M, Lima JA, Blumenthal RS
Am Heart J 2003; 146:969-977.
- "For a true exclusion of coronary artery calcifications, different reconstruction intervals have to be evaluated."
Different Reconstruction Intervals for Exclusion of Coronary Artery Calcifications by Retrospectively Gated MDCT
Sandstede JJW et al.
AJR 2006; 186:193-197(4 slice MDCT).
- "Whereas in the present study 69-77% of patients with a low pretest probability for the presence of CAD had a calcium score of 0 at one reconstruction interval at least, in only 42% of the patients could coronary artery calcification be excluded after evaluation of all reconstructions at 50%,60%,70%, and 80% of the R-R interval."
Different Reconstruction Intervals for Exclusion of Coronary Artery Calcifications by Retrospectively Gated MDCT
Sandstede JJW et al.
AJR 2006; 186:193-197(4 slice MDCT).
- "Electron-beam and multi-detector row CT scanners have equivalent reproducibility for measuring coronary artery calcium. Calcium volumes and interpolated volume scores are slightly more reproducible than Agaston scores. Reproducibility is lower for scans with misregistrations or motion artifacts."
Coronary Calcium measurements: Effect of CT Scanner Type and Calcium Measure on Rescan Reproducibility-MESA Study
Detrano RC et al.
Radiology 2005; 236:477-484.
- Factoid
- A zero coronary calcification score is associated with a high negative predictive value (nearly 100%) for excluding hemodynamically relevant CAD. The score must be 0 not 1,2 or 3 Agaston units.